

Volume 6, Issue 2 (5-2022)
EBHPME 2022, 6(2): 126-136 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ahadinezhad B, Khosravizadeh O, Vahdati F, Mohammadkhani M, Soheylirad R, Sarikhani S. Investigating the Relationship Between Management Style and Market Orientation in Qazvin University of Medical Sciences. EBHPME 2022; 6 (2) :126-136
URL: http://jebhpme.ssu.ac.ir/article-1-351-en.html
URL: http://jebhpme.ssu.ac.ir/article-1-351-en.html
Bahman Ahadinezhad 

 , Omid Khosravizadeh * , Fatemeh Vahdati , Mohammadreza Mohammadkhani , Rana Soheylirad , Sogol Sarikhani
, Omid Khosravizadeh * , Fatemeh Vahdati , Mohammadreza Mohammadkhani , Rana Soheylirad , Sogol Sarikhani
, Omid Khosravizadeh * , Fatemeh Vahdati , Mohammadreza Mohammadkhani , Rana Soheylirad , Sogol Sarikhani
Social Determinants of Health Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran , omid.khosravizadeh@gmail.com
Full-Text [PDF 643 kb]
(891 Downloads)
| Abstract (HTML) (2360 Views)
Full-Text: (591 Views)
Background: Hospital management style can affect various aspects of hospital performance. One of these aspects is the level of market orientation of the hospital. Therefore, the present study attempts to answer whether management style makes a difference in the degree market orientation of hospitals or not.
Methods: This research is a descriptive-analytical and cross-sectional study conducted in 2020. About 420 people were selected by stratified sampling out of the six medical centers' staff in Qazvin, Iran. A total of 411 people (97.86 %) completed the questionnaires. The collected data were analyzed using STATA15 and SPSS16 software. Robust regression analysis was used to estimate the role of management style in the level of market orientation of hospitals. Mean variables were analyzed using one-way analysis of variance and post hoc test.
Results: The score range of the variables was from 1 to 5. Autocratic and delegating styles obtained the highest average (3.22 ± 0.54) and the lowest average (2.87 ± 0.70), respectively. Among the dimensions of market orientation, customer orientation had the highest average (3.32 ± 0.84), while competitor orientation obtained the lowest average (2.80 ± 0.86). The average score of market orientation was 2.88 ± 0.65. A statistically significant difference between hospitals was observed in terms of participative and delegating styles (P-value < 0.05). In addition to market orientation, there was a statistically significant difference between hospitals (P-value < 0.05). The regression coefficient between the level of the hospital market orientation and the participative and delegating styles was 0.10 and 0.09
, respectively (P-value < 0.05). In contrast, the regression coefficient between autocratic style and level of market orientation was estimated to be -0.76.
Conclusion: It can be concluded that managers should use more participatory and delegating styles to increase the market orientation of the studied hospitals.
Key words: Management style, Market orientation, Hospital, Qazvin
avoid financial instability in the long run. The entry of private hospitals and social security hospitals into the market of high-income services such as profitable surgeries has put pressure on the revenues of public hospitals. In this situation, public hospitals should meet the preferences and needs of high-income groups in the best possible way and provide effective access to hospital services for the middle and lower-income groups of society by capturing the lucrative service market. The realization of this importance depends on the teaching and medical centers moving towards market orientation. Market orientation is defined as the values and beliefs in a hospital that place the patient at the center of hospital thinking, strategy, and operations and create the behaviors necessary to produce superior value for patients and meet society's current and future medical needs (1)
On the other hand, market orientation is one of the competencies that allow the hospital to have an advantage over competing hospitals (2). Contrary to some health policymakers' beliefs, university hospitals must meet the demand of high-income groups of society to strengthen revenue generation and long-term financial sustainability. Market orientation can affect the various performance indicators of an organization (3-5). Mohammadi (6), in his study in private hospitals in Isfahan, concludes that market orientation through brand identity affects hospital performance. Amangala and Wali's (7) study shows a positive relationship between market orientation and service quality. Market orientation in an organization can be both a cultural issue and a managerial issue (8). Therefore, the dominant management style can be one of the critical determinants of the hospital's market orientation. According to management theories, the hospital manager can promote a market-oriented culture by creating insight, guidance, and coordination. To promote market orientation, the manager must strengthen the customer-centric culture, attention to the competitor, and coordination between the functions of different departments (1). Hospital management can lead the hospital to be market-oriented by implementing patient-centered mechanisms, creating strategic thinking, and arranging different units in the same line. To strengthen market orientation, management must establish prerequisites such as creating market intelligence and spreading this intelligence throughout the hospital, and responding to the market based on this intelligence (9). The management style used by the manager can strengthen or weaken the hospital's market-oriented culture and behavior. Abolfazli et al. (10) concluded that companies with a high degree of market orientation use an entrepreneurial management style, while companies with a low degree of entrepreneurship and market orientation use an administrative and conservative management style. Harris & Ogbonna (11) also found a significant positive relationship between participatory style and market orientation. Other studies indicate that the positive attitude of senior managers and their emphasis on the importance of market orientation, their experience in marketing, their perception of environmental changes, their level of education, employee orientation, and risk-taking have a positive
effect on the level of market orientation of
the organization (12-17). Neglecting market orientation may have negative consequences such as reduced demand for services and reduced hospital revenue (3). Therefore, determining the type of management style that strengthens market orientation in the hospital is a prerequisite for increasing revenue. This study aimed to determine the role of management style in the level of
market orientation of Qazvin University of Medical Sciences hospitals. The findings of this study can add valid empirical evidence to the hospital management literature.
Materials and Methods
This study is descriptive-analytical research based on the survey of employees' opinions working in the Qazvin University of Medical Sciences hospitals in 2020.
Participation
In multivariate regression analysis, the sample number (observations) ratio to independent variables should not be less than 5. Otherwise, the results of the regression equation will not be very generalizable. A more conservative ratio of 10 observations per independent variable is also suggested. Considering 15 observations for each predictor variable in the multiple regression analysis with the standard method of least squares is an accurate guide. So, in general, the sample size can be determined between 5 to 15 observations per measured variable in the structural equation modeling methodology:
5Q < n < 15Q
Where Q is the number of variables observed or the number of items (questions) of the questionnaire, and n is the sample size (18). Considering that in this study, the sum of the questionnaire items is equal to 42, and considering 10 samples per item, the final sample size was obtained 420. 420 people were selected from the 6 Educational and Medical Centers of Qazvin University of Medical Sciences as the optimal sample size by stratified random sampling. In this way, the share of clusters (hospitals) in the total sample size was determined. In the next step, the subjects were randomly selected in each hospital. The inclusion criteria included willingness, satisfaction, and ability to participate. In the case of exclusion of samples, an alternative individual would be selected.
Measurement tools
Market orientation questionnaire
The market orientation of hospitals was measured using the Ahmad and Iqbal (2013) questionnaire (19). In this questionnaire, the hospital staff judges the frequency of each of the market orientation items in the hospital based on individual observation or perception and answer each of the questions on a Likert scale. This questionnaire has three dimensions: Customer orientation (6 items), competitor orientation (5 items), and inter-functional coordination (5 items). Each question is scaled through a very low (1) to very high (5). A score below 3 indicates that the hospital's market orientation level is below average and weak. A score of 3 to 4 means an above-average market orientation level, and a score above 4 indicates that the hospital has a high level of market orientation. The content validity of this questionnaire was confirmed through a survey of hospital management professors and hospital managers. The Cronbach's alpha coefficient was obtained 0.93.
Management style questionnaire
Data on management style was collected using the Clark management style questionnaire (20). In this questionnaire, hospital staff assess the frequency of each item of management style based on individual observation or perception in the hospital and answer each of the questions on a very low (1) to very high (5) level. The questionnaire consists of three styles: Autocratic management (10 items), participative management (10 items), and delegating management (10 items). Any style that achieves a higher mean (close to 5) reflects the dominant management style in the hospital. The content validity of this questionnaire was examined through a survey of hospital management professors and hospital managers, and its Cronbach's alpha coefficient was calculated at 0.92.
Data collection and analysis
After getting permission from the research deputy and receiving an ethics code, the researcher went to the studied hospitals, explained the research goals and the questionnaire structure for the samples, and then, the staff filled the questionnaires with informed consent. Robust regression analysis was used to estimate the role of management style in the level of market orientation of hospitals. In order to consider the unobservable heterogeneity between hospitals and to neutralize the effect of confounding variables specific to each hospital, the dummy variable was used for each hospital. The collected data were analyzed using STATA15 and SPSS 16 software. One-way analysis of variance was used to compare the scores of market orientation and management style among hospitals. Dummy regression was used to estimate the effect of management styles and unobservable heterogeneity of hospitals on market orientation. The regression model of the effect of management style on the level of market orientation of hospitals is as follows:

In the above model, LMO shows the logarithm of the market orientation score of the hospitals. Hi is a dummy variable that captures the unobservable effects of hospital i on the market orientation level. LAU, LPA, and LDE also show autocratic, participative, and delegating styles, respectively. It is noteworthy that beta coefficients in the high regression model show the percentage of reaction of market orientation to the percentage of change in explanatory variables.
The present study was approved by the ethical committee of Qazvin University of Medical Sciences (ethics code: IR.QUMS.REC.1399.062). After selecting the eligible participants, the researcher was introduced, and the study objectives were elaborated for the participants. The informed written consent was obtained from the subjects, and they were assured that their information would remain confidential.
Results
A total of 411 people (97.86 %) completed the questionnaires. According to the results of Table 1, most of the respondents (74.20 %) were women belonging to the clinical group (73.70 %) and had a bachelor's degree (66.70 %). Also, the average age of study participants was 36 years, and their average work experience was 11 years.
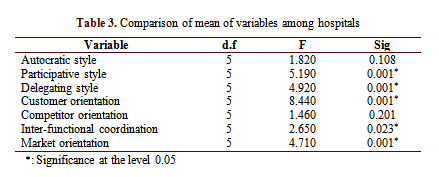
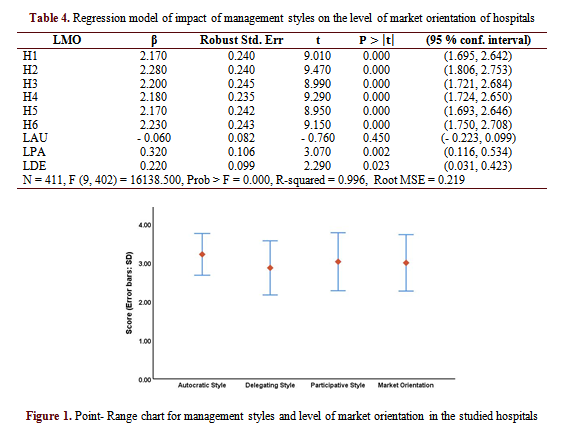
Based on Table 2 and Figure 1, the autocratic style with the highest average (3.22 out of 5) has been reported as the dominant management style. In contrast, the delegating style obtained the lowest average (2.87 out of 5). The average score of the participative style was approximately 3. Among the dimensions of market orientation, Customer orientation had the highest average (3.32 out of 5), while competitor orientation obtained the lowest average (2.80 out of 5). The average score of market orientation was 2.88 out of 5.
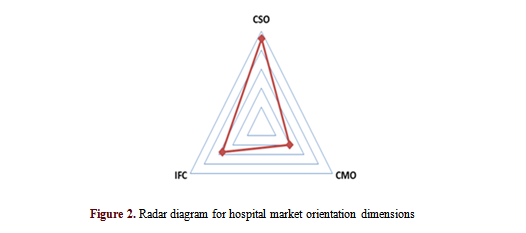
Figure 2 displays the radar diagram for the market orientation dimensions. Three dimensions of market orientation form the three vertices of this triangle. If the radar diagram fits perfectly on the triangle, it means that the hospital is at a high level in terms of market orientation. As can be seen, the diagram stretches to the dimension of customer orientation, and the other vertex of the radar triangle is stretched to inter-functional coordination.
Table 3 shows the results of comparing the mean of variables between the studied hospitals. A statistically significant difference between hospitals was observed in terms of participative and delegating styles (P-value < 0.05). It is noteworthy that hospitals did not show any statistically significant differences from each other in terms of autocratic style. In terms of market orientation, there was a statistically significant difference between hospitals (P-value < 0.05). In terms of competitor orientation, no statistically significant difference was observed between hospitals.
According to Table 4, the regression estimations show that β coefficient between the level of the hospital market orientation and the participative and delegating styles is 0.10 and 0.09, respectively (P-value < 0.05). In contrast, the regression coefficient between autocratic style and level of market orientation was estimated to be - 0.76. In addition, the unobserved hospital-specific effects are also statistically significant (P-value < 0.05).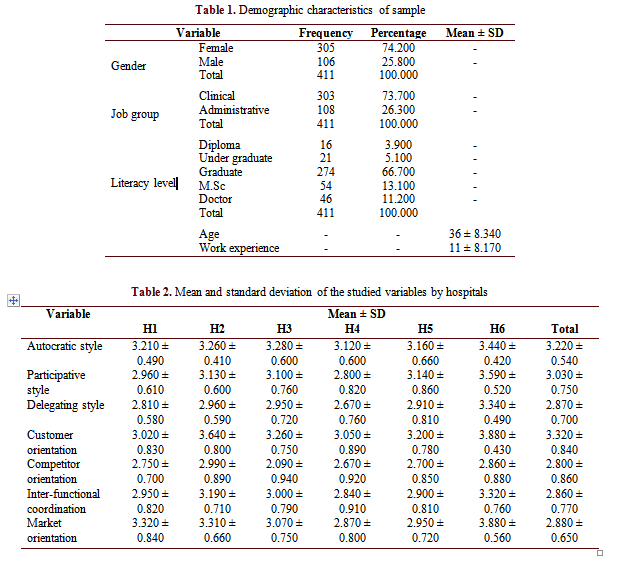
Discussion
The impact of management styles on hospitals' degree of market orientation can be a challenging discussion for scientific literature. As far as we know, our study is the first research in Iran that examines the effect of management style on the degree of market orientation of the hospital. Our analysis showed that autocratic management is the dominant style in the studied hospitals. The overall level of market orientation in the studied hospitals was below average. However, some of the studied hospitals had above-average market orientation, and the difference between the hospitals was statistically significant. Yaghoubi et al. (21) conducted a study in private hospitals in Isfahan and found that the private hospitals' market orientation was lower than average. Our findings also revealed that hospitals were above average only in terms of customer orientation and the difference in customer attention between these centers was statistically significant. As in our study, the research of Alhayari et al. (22) in one of the public hospitals of Bushehr also showed that the axial patient of nurses was above average. Findings of Golparvar and Nadi's study (23) in Isfahan medical hospitals also showed that nurses' customer-oriented behavior was above average. According to other results of our study, almost all hospitals were in a weak position concerning competitor attention, and there was no statistically significant difference between them in terms of the central competitor. In the study of Yaghoubi et al. (21), the studied hospitals scored lower than average in terms of competitor attention. One of the reasons for the lack of attention to competitors in the hospitals studied could be that these centers have not yet felt the competitive pressure created in the hospital services market due to their near-monopoly position. In other words, in these hospitals, competitors' activity is not regularly monitored, so they do not react to the movements of rival hospitals quickly. Neglecting the movements of competitors can reduce the demand for services of these hospitals. Rival hospitals try to attract rich and complementary insured patients through various strategies such as diversification of services. It reduces the quality of revenues generated in public hospitals. Also, the score of inter-functional coordination in hospitals was lower than average. However, some hospitals were above average, and the observed difference between hospitals was statistically significant. The low coordination between tasks may be because the information obtained from the hospital market may not be shared within hospitals. Employees
of different departments are not involved in developing strategies for the hospital market boom. Furthermore, it can be said that maybe not all activities are integrated to do things better. Weak market orientation and its dimensions can reduce their revenue generation by weakening the performance of hospitals. Various studies have shown the relationship between market orientation and hospital performance (24, 25). Mohammadi (26), in his study in private hospitals in Isfahan, concludes that market orientation through brand identity affects hospital performance. Our findings showed that the management style in the studied hospitals is more autocratic, and there is no statistically significant difference between hospitals in terms of using this style. While in terms of using participatory and delegating styles, there was a statistically significant difference between the studied hospitals. Also, based on the results, the managers of the studied hospitals use delegating style less than other styles. Less use of this style was seen in all studied hospitals. In a study conducted by Arab et al. (6) in hospitals of Qom province, authors concluded that the leadership styles of heads and managers of hospitals are advisory based on their answers, but from the point of view of staff, managers and heads have authoritarian-benevolent styles. In other words, considering the perspective of employees, bosses, and managers related to hospital management, they have less partnership with staff than they believe. In another study conducted among nursing managers of teaching hospitals in Hamadan, researchers concluded that the leadership style of nursing managers of hospitals was democratic (27). Amerion et al. (28), in their study in Tehran hospitals, found that managers of the studied hospitals have used more authoritarian-benevolent style. In another study, Mossadeghrad et al. (29) showed that hospital managers of Tehran University of Medical Sciences had used the cooperative style more in conflict management. The results of Saeedi et al.'s (30) study showed that most nurses in public and private hospitals use a relationship-oriented style, and there is no difference between hospitals in this regard. Researchers further conclude that in private and public hospitals in Ahvaz, there is no autocratic management style. The style that a manager adopts is based on a combination of beliefs, ideas, norms, and values. It is impossible to offer the same management style for all hospitals because using a specific management style is a contingent decision and depends on various factors such as organizational culture, hospital expertise, hospital size, and others. In line with these results, Lejpour et al. (32), in their study, conclude that the internal characteristics of the organization such as hierarchy level, managerial orientation towards tasks and people, decision-making characteristics, decision-making environment has a positive relationship with choosing the type of leadership style. The effectiveness of each style can be specific to a defined organizational climate and culture. Our findings also revealed that the autocratic style has an insignificant reduction in the level of market orientation of hospitals. While participatory and delegating styles had a significant increasing effect on the market orientation of the studied medical centers. Abolfazli et al. (10) concluded that companies with a high degree of market orientation use an entrepreneurial management style, while companies with a low degree of entrepreneurship and market orientation use an administrative and conservative management style. In their study, Harris & Ogbonna (11) also found a significant positive relationship between participatory style and market orientation. Kohli and Jawarski (9) showed that the way of thinking of senior managers and the behavior of managers affects the spread of market orientation in the organization. Other studies show that the positive attitude of senior managers and their emphasis on the importance of market orientation, their experience in marketing, their perception of environmental changes, their level of education, employee orientation, and risk-taking have a positive effect on the level of market orientation of the organization (12-18). Winston and Dadzie (33) concluded that top managers' emphasis on market orientation has the greatest impact on market orientation development. Mohammed et al. (34) conducted a study on Ghanaian pharmaceutical companies. Their study showed a significant positive relationship between senior managers' emphasis and market orientation, while senior managers' risk aversion, formality, and conflict had a significant negative relationship with market orientation. One of the reasons for the negative impact of autocratic style on the market orientation of hospitals may be interpreted in this way that this style makes change difficult in the hospital. Since employees are not involved in decision-making processes, they resist managers' decisions and the organization's values. Quality researchers state that service organizations need to be flexible enough to respond appropriately to customer needs. To do this, managers must give employees the minimum necessary authority. However, the autocratic management style does not provide employees the necessary freedom and authority (35). It should be noted that empirical evidence regarding the impact of management styles on the market orientation of organizations such as public hospitals is minimal, and definitive conclusions on this subject need further study.
Conclusion
Our study revealed that autocratic management had been the dominant style in the studied hospitals, and there is no statistically significant difference between hospitals in terms of using this style. While in terms of using participatory and delegating styles, there was a statistically significant difference between the studied hospitals. The overall level of market orientation in the studied hospitals was below average. However, some of the studied hospitals had above-average market orientation, and the difference between the hospitals was statistically significant. Also, all hospitals obtained the lowest scores in terms of competitor orientation. Our findings also revealed that the autocratic style has an insignificant reduction effect on the level of market orientation of hospitals, while participatory and delegating styles had a significant increasing effect on the market orientation of the studied medical
centers. To capture the profitable service market, hospitals must implement a strategic plan against opponents and reorganize the roles and functions of employees in order to strengthen market orientation. It is suggested that managers be taught about the techniques and functional benefits of participative and delegating styles.
Our study had one limitation. Since we could not obtain data for all hospitals in Qazvin Province, our findings cannot be generalized to all hospitals in Qazvin. It is suggested that further studies examine the impact of ownership and specialization factors on the relationship between management style and market orientation of hospitals.
Acknowledgments
We would like to thank the managers and staff of the studied hospitals for their participation and cooperation in this study.
Conflict of interests
The authors declared that there was no conflict of interests in this study.
Author's contributions
Khosravizadeh O designed research; Mohammad khani M, Vahdati F, Soheylirad R and Sarikhani S conducted research; Ahadinezhad B analyzed data; and wrote the paper. All authors read and approved the paper.
Funding
Qazvin University of Medical Sciences approved and funded this study.
Methods: This research is a descriptive-analytical and cross-sectional study conducted in 2020. About 420 people were selected by stratified sampling out of the six medical centers' staff in Qazvin, Iran. A total of 411 people (97.86 %) completed the questionnaires. The collected data were analyzed using STATA15 and SPSS16 software. Robust regression analysis was used to estimate the role of management style in the level of market orientation of hospitals. Mean variables were analyzed using one-way analysis of variance and post hoc test.
Results: The score range of the variables was from 1 to 5. Autocratic and delegating styles obtained the highest average (3.22 ± 0.54) and the lowest average (2.87 ± 0.70), respectively. Among the dimensions of market orientation, customer orientation had the highest average (3.32 ± 0.84), while competitor orientation obtained the lowest average (2.80 ± 0.86). The average score of market orientation was 2.88 ± 0.65. A statistically significant difference between hospitals was observed in terms of participative and delegating styles (P-value < 0.05). In addition to market orientation, there was a statistically significant difference between hospitals (P-value < 0.05). The regression coefficient between the level of the hospital market orientation and the participative and delegating styles was 0.10 and 0.09
, respectively (P-value < 0.05). In contrast, the regression coefficient between autocratic style and level of market orientation was estimated to be -0.76.
Conclusion: It can be concluded that managers should use more participatory and delegating styles to increase the market orientation of the studied hospitals.
Key words: Management style, Market orientation, Hospital, Qazvin
Introduction
Government budget constraints have led public hospitals to constantly strive to raise more revenue to have more resources to offset their rising costs andavoid financial instability in the long run. The entry of private hospitals and social security hospitals into the market of high-income services such as profitable surgeries has put pressure on the revenues of public hospitals. In this situation, public hospitals should meet the preferences and needs of high-income groups in the best possible way and provide effective access to hospital services for the middle and lower-income groups of society by capturing the lucrative service market. The realization of this importance depends on the teaching and medical centers moving towards market orientation. Market orientation is defined as the values and beliefs in a hospital that place the patient at the center of hospital thinking, strategy, and operations and create the behaviors necessary to produce superior value for patients and meet society's current and future medical needs (1)
effect on the level of market orientation of
the organization (12-17). Neglecting market orientation may have negative consequences such as reduced demand for services and reduced hospital revenue (3). Therefore, determining the type of management style that strengthens market orientation in the hospital is a prerequisite for increasing revenue. This study aimed to determine the role of management style in the level of
market orientation of Qazvin University of Medical Sciences hospitals. The findings of this study can add valid empirical evidence to the hospital management literature.
Materials and Methods
This study is descriptive-analytical research based on the survey of employees' opinions working in the Qazvin University of Medical Sciences hospitals in 2020.
Participation
In multivariate regression analysis, the sample number (observations) ratio to independent variables should not be less than 5. Otherwise, the results of the regression equation will not be very generalizable. A more conservative ratio of 10 observations per independent variable is also suggested. Considering 15 observations for each predictor variable in the multiple regression analysis with the standard method of least squares is an accurate guide. So, in general, the sample size can be determined between 5 to 15 observations per measured variable in the structural equation modeling methodology:
5Q < n < 15Q
Where Q is the number of variables observed or the number of items (questions) of the questionnaire, and n is the sample size (18). Considering that in this study, the sum of the questionnaire items is equal to 42, and considering 10 samples per item, the final sample size was obtained 420. 420 people were selected from the 6 Educational and Medical Centers of Qazvin University of Medical Sciences as the optimal sample size by stratified random sampling. In this way, the share of clusters (hospitals) in the total sample size was determined. In the next step, the subjects were randomly selected in each hospital. The inclusion criteria included willingness, satisfaction, and ability to participate. In the case of exclusion of samples, an alternative individual would be selected.
Measurement tools
Market orientation questionnaire
The market orientation of hospitals was measured using the Ahmad and Iqbal (2013) questionnaire (19). In this questionnaire, the hospital staff judges the frequency of each of the market orientation items in the hospital based on individual observation or perception and answer each of the questions on a Likert scale. This questionnaire has three dimensions: Customer orientation (6 items), competitor orientation (5 items), and inter-functional coordination (5 items). Each question is scaled through a very low (1) to very high (5). A score below 3 indicates that the hospital's market orientation level is below average and weak. A score of 3 to 4 means an above-average market orientation level, and a score above 4 indicates that the hospital has a high level of market orientation. The content validity of this questionnaire was confirmed through a survey of hospital management professors and hospital managers. The Cronbach's alpha coefficient was obtained 0.93.
Management style questionnaire
Data on management style was collected using the Clark management style questionnaire (20). In this questionnaire, hospital staff assess the frequency of each item of management style based on individual observation or perception in the hospital and answer each of the questions on a very low (1) to very high (5) level. The questionnaire consists of three styles: Autocratic management (10 items), participative management (10 items), and delegating management (10 items). Any style that achieves a higher mean (close to 5) reflects the dominant management style in the hospital. The content validity of this questionnaire was examined through a survey of hospital management professors and hospital managers, and its Cronbach's alpha coefficient was calculated at 0.92.
Data collection and analysis
After getting permission from the research deputy and receiving an ethics code, the researcher went to the studied hospitals, explained the research goals and the questionnaire structure for the samples, and then, the staff filled the questionnaires with informed consent. Robust regression analysis was used to estimate the role of management style in the level of market orientation of hospitals. In order to consider the unobservable heterogeneity between hospitals and to neutralize the effect of confounding variables specific to each hospital, the dummy variable was used for each hospital. The collected data were analyzed using STATA15 and SPSS 16 software. One-way analysis of variance was used to compare the scores of market orientation and management style among hospitals. Dummy regression was used to estimate the effect of management styles and unobservable heterogeneity of hospitals on market orientation. The regression model of the effect of management style on the level of market orientation of hospitals is as follows:
In the above model, LMO shows the logarithm of the market orientation score of the hospitals. Hi is a dummy variable that captures the unobservable effects of hospital i on the market orientation level. LAU, LPA, and LDE also show autocratic, participative, and delegating styles, respectively. It is noteworthy that beta coefficients in the high regression model show the percentage of reaction of market orientation to the percentage of change in explanatory variables.
The present study was approved by the ethical committee of Qazvin University of Medical Sciences (ethics code: IR.QUMS.REC.1399.062). After selecting the eligible participants, the researcher was introduced, and the study objectives were elaborated for the participants. The informed written consent was obtained from the subjects, and they were assured that their information would remain confidential.
Results
A total of 411 people (97.86 %) completed the questionnaires. According to the results of Table 1, most of the respondents (74.20 %) were women belonging to the clinical group (73.70 %) and had a bachelor's degree (66.70 %). Also, the average age of study participants was 36 years, and their average work experience was 11 years.
Based on Table 2 and Figure 1, the autocratic style with the highest average (3.22 out of 5) has been reported as the dominant management style. In contrast, the delegating style obtained the lowest average (2.87 out of 5). The average score of the participative style was approximately 3. Among the dimensions of market orientation, Customer orientation had the highest average (3.32 out of 5), while competitor orientation obtained the lowest average (2.80 out of 5). The average score of market orientation was 2.88 out of 5.
Figure 2 displays the radar diagram for the market orientation dimensions. Three dimensions of market orientation form the three vertices of this triangle. If the radar diagram fits perfectly on the triangle, it means that the hospital is at a high level in terms of market orientation. As can be seen, the diagram stretches to the dimension of customer orientation, and the other vertex of the radar triangle is stretched to inter-functional coordination.
Table 3 shows the results of comparing the mean of variables between the studied hospitals. A statistically significant difference between hospitals was observed in terms of participative and delegating styles (P-value < 0.05). It is noteworthy that hospitals did not show any statistically significant differences from each other in terms of autocratic style. In terms of market orientation, there was a statistically significant difference between hospitals (P-value < 0.05). In terms of competitor orientation, no statistically significant difference was observed between hospitals.
According to Table 4, the regression estimations show that β coefficient between the level of the hospital market orientation and the participative and delegating styles is 0.10 and 0.09, respectively (P-value < 0.05). In contrast, the regression coefficient between autocratic style and level of market orientation was estimated to be - 0.76. In addition, the unobserved hospital-specific effects are also statistically significant (P-value < 0.05).
Discussion
The impact of management styles on hospitals' degree of market orientation can be a challenging discussion for scientific literature. As far as we know, our study is the first research in Iran that examines the effect of management style on the degree of market orientation of the hospital. Our analysis showed that autocratic management is the dominant style in the studied hospitals. The overall level of market orientation in the studied hospitals was below average. However, some of the studied hospitals had above-average market orientation, and the difference between the hospitals was statistically significant. Yaghoubi et al. (21) conducted a study in private hospitals in Isfahan and found that the private hospitals' market orientation was lower than average. Our findings also revealed that hospitals were above average only in terms of customer orientation and the difference in customer attention between these centers was statistically significant. As in our study, the research of Alhayari et al. (22) in one of the public hospitals of Bushehr also showed that the axial patient of nurses was above average. Findings of Golparvar and Nadi's study (23) in Isfahan medical hospitals also showed that nurses' customer-oriented behavior was above average. According to other results of our study, almost all hospitals were in a weak position concerning competitor attention, and there was no statistically significant difference between them in terms of the central competitor. In the study of Yaghoubi et al. (21), the studied hospitals scored lower than average in terms of competitor attention. One of the reasons for the lack of attention to competitors in the hospitals studied could be that these centers have not yet felt the competitive pressure created in the hospital services market due to their near-monopoly position. In other words, in these hospitals, competitors' activity is not regularly monitored, so they do not react to the movements of rival hospitals quickly. Neglecting the movements of competitors can reduce the demand for services of these hospitals. Rival hospitals try to attract rich and complementary insured patients through various strategies such as diversification of services. It reduces the quality of revenues generated in public hospitals. Also, the score of inter-functional coordination in hospitals was lower than average. However, some hospitals were above average, and the observed difference between hospitals was statistically significant. The low coordination between tasks may be because the information obtained from the hospital market may not be shared within hospitals. Employees
of different departments are not involved in developing strategies for the hospital market boom. Furthermore, it can be said that maybe not all activities are integrated to do things better. Weak market orientation and its dimensions can reduce their revenue generation by weakening the performance of hospitals. Various studies have shown the relationship between market orientation and hospital performance (24, 25). Mohammadi (26), in his study in private hospitals in Isfahan, concludes that market orientation through brand identity affects hospital performance. Our findings showed that the management style in the studied hospitals is more autocratic, and there is no statistically significant difference between hospitals in terms of using this style. While in terms of using participatory and delegating styles, there was a statistically significant difference between the studied hospitals. Also, based on the results, the managers of the studied hospitals use delegating style less than other styles. Less use of this style was seen in all studied hospitals. In a study conducted by Arab et al. (6) in hospitals of Qom province, authors concluded that the leadership styles of heads and managers of hospitals are advisory based on their answers, but from the point of view of staff, managers and heads have authoritarian-benevolent styles. In other words, considering the perspective of employees, bosses, and managers related to hospital management, they have less partnership with staff than they believe. In another study conducted among nursing managers of teaching hospitals in Hamadan, researchers concluded that the leadership style of nursing managers of hospitals was democratic (27). Amerion et al. (28), in their study in Tehran hospitals, found that managers of the studied hospitals have used more authoritarian-benevolent style. In another study, Mossadeghrad et al. (29) showed that hospital managers of Tehran University of Medical Sciences had used the cooperative style more in conflict management. The results of Saeedi et al.'s (30) study showed that most nurses in public and private hospitals use a relationship-oriented style, and there is no difference between hospitals in this regard. Researchers further conclude that in private and public hospitals in Ahvaz, there is no autocratic management style. The style that a manager adopts is based on a combination of beliefs, ideas, norms, and values. It is impossible to offer the same management style for all hospitals because using a specific management style is a contingent decision and depends on various factors such as organizational culture, hospital expertise, hospital size, and others. In line with these results, Lejpour et al. (32), in their study, conclude that the internal characteristics of the organization such as hierarchy level, managerial orientation towards tasks and people, decision-making characteristics, decision-making environment has a positive relationship with choosing the type of leadership style. The effectiveness of each style can be specific to a defined organizational climate and culture. Our findings also revealed that the autocratic style has an insignificant reduction in the level of market orientation of hospitals. While participatory and delegating styles had a significant increasing effect on the market orientation of the studied medical centers. Abolfazli et al. (10) concluded that companies with a high degree of market orientation use an entrepreneurial management style, while companies with a low degree of entrepreneurship and market orientation use an administrative and conservative management style. In their study, Harris & Ogbonna (11) also found a significant positive relationship between participatory style and market orientation. Kohli and Jawarski (9) showed that the way of thinking of senior managers and the behavior of managers affects the spread of market orientation in the organization. Other studies show that the positive attitude of senior managers and their emphasis on the importance of market orientation, their experience in marketing, their perception of environmental changes, their level of education, employee orientation, and risk-taking have a positive effect on the level of market orientation of the organization (12-18). Winston and Dadzie (33) concluded that top managers' emphasis on market orientation has the greatest impact on market orientation development. Mohammed et al. (34) conducted a study on Ghanaian pharmaceutical companies. Their study showed a significant positive relationship between senior managers' emphasis and market orientation, while senior managers' risk aversion, formality, and conflict had a significant negative relationship with market orientation. One of the reasons for the negative impact of autocratic style on the market orientation of hospitals may be interpreted in this way that this style makes change difficult in the hospital. Since employees are not involved in decision-making processes, they resist managers' decisions and the organization's values. Quality researchers state that service organizations need to be flexible enough to respond appropriately to customer needs. To do this, managers must give employees the minimum necessary authority. However, the autocratic management style does not provide employees the necessary freedom and authority (35). It should be noted that empirical evidence regarding the impact of management styles on the market orientation of organizations such as public hospitals is minimal, and definitive conclusions on this subject need further study.
Conclusion
Our study revealed that autocratic management had been the dominant style in the studied hospitals, and there is no statistically significant difference between hospitals in terms of using this style. While in terms of using participatory and delegating styles, there was a statistically significant difference between the studied hospitals. The overall level of market orientation in the studied hospitals was below average. However, some of the studied hospitals had above-average market orientation, and the difference between the hospitals was statistically significant. Also, all hospitals obtained the lowest scores in terms of competitor orientation. Our findings also revealed that the autocratic style has an insignificant reduction effect on the level of market orientation of hospitals, while participatory and delegating styles had a significant increasing effect on the market orientation of the studied medical
centers. To capture the profitable service market, hospitals must implement a strategic plan against opponents and reorganize the roles and functions of employees in order to strengthen market orientation. It is suggested that managers be taught about the techniques and functional benefits of participative and delegating styles.
Our study had one limitation. Since we could not obtain data for all hospitals in Qazvin Province, our findings cannot be generalized to all hospitals in Qazvin. It is suggested that further studies examine the impact of ownership and specialization factors on the relationship between management style and market orientation of hospitals.
Acknowledgments
We would like to thank the managers and staff of the studied hospitals for their participation and cooperation in this study.
Conflict of interests
The authors declared that there was no conflict of interests in this study.
Author's contributions
Khosravizadeh O designed research; Mohammad khani M, Vahdati F, Soheylirad R and Sarikhani S conducted research; Ahadinezhad B analyzed data; and wrote the paper. All authors read and approved the paper.
Funding
Qazvin University of Medical Sciences approved and funded this study.
Type of Study: Original article |
Subject:
Healt care Management
Received: 2021/05/24 | Accepted: 2022/05/20 | Published: 2022/07/3
Received: 2021/05/24 | Accepted: 2022/05/20 | Published: 2022/07/3
References
1. Narver JC, Slater SF. The effect of a market orientation on business profitability. Journal of Marketing. 1990; 54(4): 20-35. [DOI:10.1177/002224299005400403]
2. Agazadeh H, Mehrnoosh M. Indigenous scale of market orientation of Iranian commercial banks. Business Management Perspective. 2010; 9(2): 119-43. [In Persian]
3. Harris LC, Ogbonna E. Leadership style and market orientation: An empirical study. European Journal of Marketing. 2001; 35 (5/6): 744-64. [DOI:10.1108/03090560110388196]
4. Azar A, Taqizadeh Jurshari MR, Takhireh M. Impact of comprehensive quality management on performance banks: Mediation market orientation. Journal of Business Management Perspective. 2015; 14(22): 29-47. [In Persian]
5. Sampaio CAF, Hernández-Mogollón JM, Rodrigues RG. Assessing the relationship between market orientation and business performance in the hotel industry-the mediating role of service quality. Journal of Knowledge Management. 2019; 23(4): 644-63. [DOI:10.1108/JKM-08-2017-0363]
6. Mohammadi F. Analyzing the role of market orientation on hospitals performance with emphasis on the role of organization brand identity case study: Private hospitals in Isfahan city. Quarterly Journal of New Marketing Research. 2018; 7(4): 145-56. [In Persian] [DOI:10.22108/NMRJ.2018.108466.1523]
7. Amangala EA, Wali AF. Market orientation, service quality perception, and customer satisfaction: The role of market-sensing capabilities. Business Perspectives and Research. 2020; 8(2): 216-31. [DOI:10.1177/2278533719887453]
8. Dadashi MA, Mohammadian M, Dehdashti Shahrokh Z, Khashei V. Native model of development of market orientation of organic products in Iran. Journal of Agricultural Economics Research. 2018; 9(36): 231-58. [In Persian]
9. Kohli AK, Jaworski BJ, Kumar A. MARKOR: A measure of market orientation. Journal of Marketing Research. 1993; 30(4): 467-77. [DOI:10.1177/002224379303000406]
10. Abolfazli SA, Salar J, Rezaian A. The relationship between entrepreneurial management, market orientation and performance. Business Management Outlook (Management Outlook (Management Message)). 2015. 14(22): 123-39. [In Persian] [DOI:10.7748/nm.22.5.14.s14]
11. Harris LC, Ogbonna E. Strategic human resource management, market orientation, and organizational performance. Journal of Business Research. 2001; 51(2): 157-66. [DOI:10.1016/S0148-2963(99)00057-0]
12. Brettel M, Engelen A, Heinemann F, Vadhanasindhu P. Antecedents of market orientation: A cross-cultural comparison. Journal of International Marketing. 2008; 16(2): 84-119. [DOI:10.1509/jimk.16.2.84]
13. Chakravorti S. Market orientation of firms in international markets. A review research article presented in the 3rd Annual International Conference on Enterprise Marketing and Globalization (EMG 2013): Organized by Global Science and Technology Forum in Singapore; 2013. 22-3. [DOI:10.5176/2251-2098_EMG13.04]
14. Bengtsson S, Solheim BG. Enforcement of data protection, privacy and security in medical informatics. Proceedings of the 7th World Congress on Medical Informatics; 1992 Sep 6-10; Geneva, Switzerland. Amsterdam: North-Holland; 1992: 1561-5
15. Horng AH, Chen AC. Market orientation of small and medium sized firms in Taiwan. Journal of Small Business Management. 1998; 36(2): 79-85.
16. Kirca AH, Jayachandran S, Bearden WO. Market orientation: A meta-analytic review and assessment of its antecedents and impact on performance. Journal of Marketing. 2005; 69(2): 24-41. [DOI:10.1509/jmkg.69.2.24.60761]
17. Ranjbarian B, Kaboli MR, Rojuee M, Sanaei A. An analysis of antecedent and consequences of market orientation for Iran's insurance industry. Journal of Management Research. 2012; 4(1): 1-25.
18. Hooman, HA. Structural equation modeling book using LISREL software. 6 th. Tehran: Organization for the study and compilation of University Humanities; 2014. 1-352.
19. Ahmad N, Iqbal N. The impact of market orientation and brand orientation on strengthening brand performance: An insight from the beverage industry of Pakistan. International Review of Management and Business Research. 2013; 2(1): 128-32.
20. Clark. D (1998): Leadership Style Survey. Retrieved in Feb. 12, 2008, Available from URL: http://www.nwlink.com/~donclark/leader/survstyl.html. Last access: 21 December, 2021.
21. Yaghoubi M, Agharahimi Z, Javadi M, Bahadori MK. The relationship between market orientation, organizational structure and system approach in private hospitals of Isfahan. Daneshvar. 2013; 21(108): 1-12. [In Persian]
22. Allahyari Bouzanjani A, Abbasi A, Alipour F, Khosravaninezhad F. Effect of nurses perceptions on the quality of services received by managers on their customer-oriented behaviors (patient centered care). Quarterly Journal of Nursing Management. 2016; 5(3): 53-61. [In Persian] [DOI:10.29252/ijnv.5.3.4.53]
23. Golparvar M, Nadi MA. Perceptions of Justice with Customer - Oriented Behaviors among Nurses. JHA. 2009; 12 (35): 61-82. [In Persian]
24. Hwang YI, Chung S. Market orientation, social responsibility, and performance in Korea's healthcare industry. International Journal of Healthcare Management. 2018; 11(4): 325-32. [DOI:10.1080/20479700.2017.1404728]
25. Kumar PN, Jacob A, Thota S. Impact of healthcare marketing and bradning on hospital service. Int J Res Foundation Hosp Healthc Adm. 2014; 2(1): 19-24. [DOI:10.5005/jp-journals-10035-1010]
26. Arab M, Tajvar M, Akbari FA, Zeraati H. Styles of hospital administration and features of managers and staffs. Journal of Health Faculty and Health Research Institiotion. 2006; 4(3): 43-52. [In Persian]
27. Bikmoradi A, Hamidi Y, Soltanian AR, Abdi F. Correlation of nurse managers' demographic characteristics with their leadership styles in educational hospitals of Hamadan City in 2014. Sci J Hamadan Midwifery Fac. 2016; 24(3): 159-66. [In Persian] [DOI:10.21859/nmj-24033]
28. Amerioun A, Hosseini Shokouh SM, Karimi Zarchi AA, Mahmoudi N. Hospital manager's leadership style from staff's viewpoint and its relationship with hospital indicators. Iranian Journal of Military Medicine. 2011; 13(3): 125-32. [In Persian]
29. Mosadeghrad AM, Arab M, Mojbafan A. Study of conflict management styles in Tehran University affiliated hospitals. Journal of Health Based Research. 2016; 2(1): 1-13. [In Persian]
30. Saeidi Gh, Elahi N, Neysi A, Latifi SM. A survey on leadership styles of head-nurses and clinical competency of nurses in public and private hospitals of Ahvaz in 2014: A short report. J Rafsanjan Univ Med Sci. 2016; 15(1): 81-90. [In Persian]
31. Teepapal T. The determinants of subordinates' perceived leadership styles in small and medium enterprises in Thailand. AU Journal of Management. 2013; 11(1): 17-27.
32. Lojpur A, Aleksić A, Vlahović S, Bach MP, Peković S. Examining determinants of leadership style among montenegrin managers. Naše Gospodarstvo/ Our Economy. 2015; 61(1): 13-24.
33. Winston E, Dadzie KQ. Market orientation of Nigerian and Kenyan firms: The role of top managers. The Journal of Business and Industrial Marketing. 2002; 17(6): 471-80. [DOI:10.1108/08858620210442820]
34. Mohammed A, Kastner A, Yeboah J. Antecedents, environmental moderators and consequences of market orientation: A study of pharmaceutical firms in Ghana. Journal of Medical Marketing: Device, Diagnostic and Pharmaceutical Marketing. 2010; 10(3): 231-44.
35. Clark RA, Hartline MD, Jones KC. The effects of leadership style on hotel employees' commitment to service quality. Cornell Hospitality Quarterly. 2009; 50(2): 209-31. [DOI:10.1177/1938965508315371]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
