

Volume 6, Issue 4 (10-2022)
EBHPME 2022, 6(4): 273-284 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seyedin H, Afshari M, Isfahani P, Hasanzadeh E, Radinmanesh M, Corani Bahador R. Strategies for Reducing Induced Demand in Hospitals Affiliated with Iran University of Medical Sciences: A Qualitative Study. EBHPME 2022; 6 (4) :273-284
URL: http://jebhpme.ssu.ac.ir/article-1-407-en.html
URL: http://jebhpme.ssu.ac.ir/article-1-407-en.html
Hesam Seyedin 
 , Mahnaz Afshari , Parvaneh Isfahani , Ebrahim Hasanzadeh , Maryam Radinmanesh , Rasoul Corani Bahador *
, Mahnaz Afshari , Parvaneh Isfahani , Ebrahim Hasanzadeh , Maryam Radinmanesh , Rasoul Corani Bahador *
, Mahnaz Afshari , Parvaneh Isfahani , Ebrahim Hasanzadeh , Maryam Radinmanesh , Rasoul Corani Bahador *
Social Determinants of Health Research Center, Saveh University of Medical Sciences, Saveh, Iran , rasoul.bahador@gmail.com
Full-Text [PDF 376 kb]
(406 Downloads)
| Abstract (HTML) (641 Views)
Full-Text: (117 Views)
Background: Induced demand is a major challenge for health systems worldwide. It increases costs, especially for patients. The purpose of this study is to identify strategies for reducing induced demand for health care in hospitals affiliated with the Iran University of Medical Sciences (IUMS).
Methods: This was a qualitative study conducted in 2018. The authors conducted in-depth, semi-structured interviews with 20 participants, including IUMS faculty members, physicians, public hospital managers, patients, and researchers with academic and practical experience. Inductive content analysis was used to analyze data. Data analysis was performed in MAXQDA10.
Results: Overall, the authors extracted 24 subthemes from the interviews and classified them into the health system, insurer, healthcare provider, and healthcare recipient. They are key factors regarding the induced demand for healthcare in the public hospitals under study.
Conclusion: Reducing induced demand for healthcare requires concerted actions by health policymakers and managers at the level of the health system, insurers, healthcare providers, and healthcare recipients. Therefore, policymakers and managers of the health system should take appropriate measures such as the development of guidelines and protocols by different departments, especially the emergency department, classification (primary, secondary, and tertiary care), and referral system. They expand the monitoring role of insurance companies (transforming the payment system into the global diagnosis-related group) to reduce the induced demand for health.
Keywords: Induced demand, Hospital, Strategy
Productivity and cost containment have become increasingly vital in healthcare. This is because of the complexity of the provision of care, rising costs of healthcare, increasing demand for care, and limited financial and human resources (1, 2). Inappropriate allocation of resources within the health sector and technical and management inefficiencies within hospitals can lead to a significant waste of resources. Improving hospital efficiency allows for the provision of higher-quality care and better use of available resources. This is especially important at a time when shortage of healthcare funds is a worldwide challenge. One example of inefficiency within the health sector and individual hospitals is supplier-induced demand which imposes additional costs on patients and insurance companies as well as a heavy financial burden on the health system (3).
Induced demand is a long-debated topic in the field of health economics. It is defined as the change in the demand for healthcare associated with the discretionary influence of providers, especially physicians, over their patients (3). As a complex and multidimensional phenomenon, induced demand is a major challenge for health systems worldwide. It creates an imbalance between needs and available resources; thus, increasing patients’ share in healthcare costs and Catastrophic Health Expenditure (CHE) (4).
The concept of supplier-induced demand has been addressed in the health economics
literature for 30 years, and it is one of the
controversial topics in this field. Various definitions have been given for supplier-induced demand. For example, induced demand from Pauly's point of view is" a demand which takes advantage of data more than patients regarding health services and provides excessive care with questionable value" (5). Crane also defines induced demand: "inducing the provision, care or sale of unnecessary services to clients of the health system, which is related to the exercise of power by service providers, is termed induced demand" (6).
This type of demand can be in the form of increasing the number of services or changing the services provided to patients. Induced demand for health services can be related to two types of extensive medical services such as consultation and visits or referrals to diagnostic centers (7). The premise of the supplier-induced demand hypothesis is based on the assumption of asymmetric information between the doctor and the patient. A patient does not have enough information to assess the quantity and quality of services provided. Therefore, the doctor acts as a consultant to the patient and provides medical care to her/him. The doctor can have a significant effect on the type and quality of services provided (8). For example, a study in the United States showed that there was a significant relationship between the number of doctors and the price of services, and the number of consultations and visits (9).
Induced demand undermines the efficient allocation of national resources, even when all the costs are paid by patients. This situation can disturb the balance of supply and demand in the healthcare market while imposing additional burdens on the patients. At times, incorrect diagnosis and/or treatment lead to medical complications for care recipients (10, 11) From a health policy perspective, induced demand raises two main concerns. On the one hand, it increases health expenses and puts a burden on government budgets. On the other hand, it affects efficiency, since a higher share of a nation’s resources is devoted to healthcare with few benefits (7). Moreover, induced demand for care could result in a massive economic loss at the national level, especially when the government subsidizes medical services and drugs (12).
Romer and his colleague's studies were the first research on supplier-induced demand, known as Romer's Law in the healthcare market. This law states, “a hospital bed built is a filled bed”. Although this theory has been proposed for demanding hospital services, it can extend to the doctors' services as well (13). The service provider has no motivation to provide services at an optimal level, and providing unnecessary services causes a waste of resources and inefficiency. This is because they impose additional costs on patients to increase income or anything in their interests (14).
The probability of induced demand occurrence and the intensity of its effects can be the result of the interaction of a wide range of factors that can influence patients' behavior (15). Patients can be influential in creating induced demand from health service providers. Factors such as medical history and physical and mental condition can show patients' preferences and values. Patients have unlimited preferences and desires for health services (7). Moreover, systemic factors can also be another cause of induced demand for health services. These factors can facilitate the creation of induced demand in different ways such as increasing profits, increasing sales of services, and marketing (16). Various reasons lead to an induced demand in the healthcare system. Therefore, the purpose of the present
research is to identify strategies for reducing
induced demand regarding healthcare in Iran as a useful step toward efficient management of the health system, cost containment in the health sector, and, eventually, improved quality of care.
Materials and Methods
This qualitative research was conducted in 2018 in hospitals affiliated with the Iran University of Medical Sciences (IUMS). By conducting semi-structured interviews, researchers identified solutions to reduce induced demand in the health system. The researchers arranged the time and place of the interviews with the participants in advance. Before starting interviews, while explaining the study objectives and the confidentiality of the data, participants completed an informed consent form. Then, they were asked for permission to tape-record their conversations. In addition, researchers tried to obtain complete information about their experiences and opinions about the research objectives.This was done by communicating and interacting effectively with the participants and guiding them to the desired topic. Moreover, during the interviews, notes were taken to confirm the correctness of the data. This was done by restating the important points and summarizing the participants' responses. The interviews were conducted individually and as much as possible in a calm environment without the presence of others.
An interview guide was developed based on the objectives of the research and the literature. Three pilot interviews were conducted to optimize the questions, improve the interviewer’s communication skills, and increase the validity of the research. The participants were selected by experts related to the subject. Accordingly, policymakers, managers and doctors, and employees of health and medical organizations, and faculty members of medical sciences universities across the country with at least 3 years of experience in managerial, executive, and scientific activities were included.
Interviewees were selected using purposive and snowball sampling techniques and interviews continued until saturation was reached (20 interviews). Interviews were arranged in advance and at the participants’ workplaces. On average, each interview lasted about 36 minutes (30-45 minutes). Interviewees were coded with the letter “M”. Transcripts were 4 to 10 pages long.
Data analysis was done simultaneously with their collection. Immediately after each interview, the authors typed the recorded conversations. Brown and Clark's (17) six-step thematic analysis method, including understanding the data, identifying primary codes, searching for themes, reviewing themes, defining themes, and preparing a report, was used to analyze the qualitative data of this study. Data analysis was performed in MAXQDA10.
The research team increased the validity and generalizability of the research results. This was done using measures such as sampling with maximum diversity; conducting pilot interviews; long contact with the research environment; spending enough time to conduct interviews; examining the issue from different angles; collecting as much information and evidence as possible, collecting and analyzing documents; comparing the obtained information; sending the findings to a sample of the interviewees and including their additional comments; exchanging opinions with peers and scrutinizing the research environment and the steps of the research. In addition, pilot interviews, careful explanation of the interview procedure, triangulation of the obtained data, and gathering more information and evidence were measures the authors took to ensure objectivity. Ethical considerations included complying with the IUMS ethics code (IR.IUMS.REC 1396.30888), acquiring informed consent, asking permission to record interviews, maintaining confidentiality, and avoiding bias in data collection, analysis, and reporting.
Results
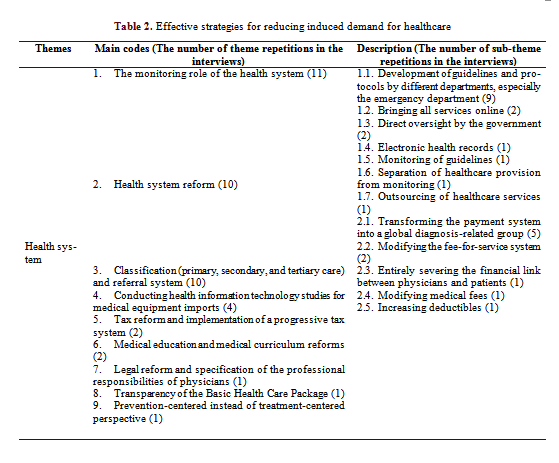
20 faculty members, physicians, public hospital managers, patients, and researchers with academic and practical experience participated in this study (Table 1). 4 themes and 24 subthemes on strategies for the reduction of induced demand for healthcare were extracted from the interviews. The main themes included the health system, the insurer, the healthcare provider, and the healthcare recipient (Table 2).
Theme 1: Strategies related to the health system
The interviewees offered nine strategies related to the health system which could be effective for reducing induced demand for health care: monitoring the role of the health system; health system reform; classification and referral system; conducting health information technology studies for medical equipment imports; tax reform and implementation of a progressive tax system; medical education and medical curriculum reforms; legal reform and specification of the professional responsibilities of physicians; transparency of the basic healthcare package; and prevention-centered instead of treatment-centered perspective. Some of the comments made by the interviewees are as follows:
“Monitoring and investigating should occur in the current situation. The authors have to ensure that the right technologies are imported, and also make sure that they are used correctly. For example, anyone with a knee injury can receive an MRI, but is it really necessary? It depends on the patient. Classification of care in the private sector was excluded from the Fourth Development Plan, and about 250 MRI licenses were issued for Tehran. But the Fifth Development Plan included this classification; wrong licenses were issued and prices went up. This imposed a massive financial burden on the system.” (M1) (monitoring role of the health system)
“The best thing is to sever the financial link between the physician and the patient completely. I mean, the patient doesn’t pay out-of-pocket, and the insurance company covers the costs, especially private insurance companies because public insurance companies don’t really care much about the number of services provided. In a nutshell, there should be no financial link between physicians and patients, and coverage of services should be delegated to private insurance companies.” (M2) {payment system reform)
“Payment reforms can be very helpful; we should have the right price for services.” (M3) (payment system reform)
“First and foremost, we have to adjust the Fee-For-Service (FFS) system, which is currently the dominant payment system in the country. If the share of FFS in the salary is higher, the likelihood of inducing demand increases. In developed countries, FFS constitutes only a small part of a person’s salary to motivate the provision of care. The opposite is true in Iran. FFS makes up a large part of the person’s salary. In order to motivate physicians without encouraging inducement of demand, FFS shouldn’t be greater than their salary.” (M4) (payment system reform)
“We’re a Third World country, so we should have some mechanisms for evaluating the import of certain technologies. When too many MRI machines are imported, owners are more likely to encourage physicians to induce demand for its use. Those mechanisms should provide oversight and prevent this.” (M5) (conducting IT studies regarding health for equipment imports)
“Our tax system should be transparent. It can foster certain behaviors. Our tax system should be linked to our information systems. Some countries implement a progressive tax system for physicians. For example, those earning $100,000 are taxed at a certain rate, those earning $150,000 are taxed at a slightly higher rate, and so on. Sometimes income tax rate reaches 90 %, and the individual has no incentive to provide more services. Progressive tax can be very beneficial in preventing induced demand. Of course, there has to be an oversight to deter physicians from selecting easy cases and rejecting more complex ones.” (M4) (tax reform and implementation of a progressive tax system)
“The next strategy is curriculum reform. General Practitioners (GPs) are capable of performing a lot of tasks. But in Iran, there are GPs who can hardly perform basic tests. If authorities manage to update general practice education programs, they’ll be able to reduce costs significantly, especially at a time when the country is struggling with sanctions and other problems.” (M7) (medical education and medical curriculum reforms)
“There should be transparency in our Basic Health Care package. Priorities should be based on the incidence of diseases and disabilities and the mortality rate. Interventions should be practical; for example, when a healthcare package is to be proposed, it must have a healthcare standard attachment, a clinical guidelines attachment, a health system attachment, and an accreditation system attachment. Ensuring these is a big step toward health system reform.” (M8) (transparency in the Basic Health Care package)
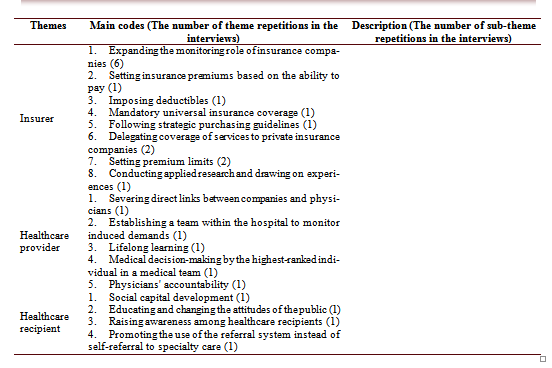
Theme 2: Strategies related to the insurer
Eight strategies related to the insurer were identified by the interviewees: expanding the monitoring role of insurance companies; setting insurance premiums based on the ability to pay; charging deductibles; mandatory universal insurance coverage; following strategic purchasing guidelines; delegating coverage of services to private insurance companies; setting premium limits; and conducting applied research and drawing on past experiences. Some of the comments made by the interviewees are as follows:
“The health system and the insurance system must have strict regulations on monitoring, and conflicts of interest must be managed.” (M9) (expanding the monitoring role of insurance companies)
“The problem is that paragraph B of article 38 in the fifth development plan, and paragraph A of article 70 in the sixth development plan, which highlights mandatory universal health insurance coverage, haven’t been implemented yet. This is one of the main pillars of the health system. These laws can clarify our policies and inform us about vulnerable people who must be covered, people who must contribute to national insurance, and people who must pay both premium and progressive tax. Then, we can talk about the financial relationship between physicians and patients. It all comes down to the paying ability of our insurance companies and competition in the market. Many countries have reduced the financial relationship between physicians and patients to zero. In many countries such as Thailand and Turkey, a physician is the team supervisor. Based on our healthcare resources, government assistance, and patients’ deductibles, we can determine the extent of support and coverage that can be provided. We must take action to provide social support for patients and make sure that they don’t suffer high medical expenditures.” (M10) (setting insurance premiums based on the ability to pay)
“Insurance companies are the biggest stakeholders and must make sure that this notion is understood within the health system. They must recognize that induced demand will lead to a budget deficit and bankruptcy, just like the Social Security Insurance Organization which has declared bankruptcy. This organization doesn’t charge any deductibles on its affiliated hospitals, which has resulted in a great deal of induced demand. There are cases of multiple revisits in one month with the same diagnosis and the same drugs, which are sometimes not even used.” (M11) (charging deductibles)
“If insurance companies play an active role and act according to strategic purchasing guidelines, induced demand can be controlled to a large extent, which is especially important now that lack of resources is more strongly felt more than ever.” (M12) (following strategic purchasing guidelines)
Theme 3: Strategies related to the healthcare provider
Five effective strategies related to the healthcare provider were identified by the interviewees: severing direct links between companies and physicians; establishing a team within the hospital to monitor induced demands; lifelong learning; medical decision-making by the highest-ranked individual in a medical team; and physician's accountability. Some of the comments made by the interviewees are as follows:
“Preventing direct links between companies and physicians can be very advantageous.” (M13) (severing direct links between companies and physicians)
“A strong team or committee can be established within the hospital, consisting of several key individuals such as the CEO and managers of different departments to address the unnecessary services that are provided and come up with mechanisms to monitor and prevent it.” (M14) (establishing a team within the hospital to monitor induced demands)
“Physicians who graduate from medical schools no longer receive education and many of them continue working based on the knowledge acquired in the past. Despite the fast changes and advances in medical science, they keep relying on outdated information. Effectiveness of some treatments can be calculated using software, but they don’t receive training and are not updated; therefore, induced demand still exists.” (M15) (lifelong learning)
“Clinical decisions should be made by the highest-ranked physician in the medical team to increase physicians’ confidence and allow them to work without being unnecessarily concerned about legal issues.” (M16) (medical decision-making by the highest-ranked individual in a medical team)
Theme 4: Strategies related to the healthcare recipient
According to the interviewees, there are four effective strategies related to the healthcare recipient which can help reduce induced demand. They include social capital development, educating and changing the attitudes of the public, raising awareness among healthcare recipients, and promoting the use of the referral system instead of self-referral to specialty care. Some of the comments made by the interviewees are as follows:
“The issue of social capital is very important; it influences the behavior of healthcare consumers, the behavior of healthcare providers, and the behavior of social mechanisms. This requires strengthening certain things such as associations and seminars.” (M17) (social capital development)
“We must embed public health into culture through mass media instead of encouraging unhealthy lifestyles. These issues can also be promoted through digital media or by distributing pamphlets in organizations, schools, universities, etc.” (M18) (educating and changing attitudes of the public)
“Another way is to raise awareness among healthcare recipients about induced demand and encourage them to consult with informed individuals.” (M19) (raising awareness among healthcare recipients)
The purpose of this research was to identify effective strategies for reducing induced demand in hospitals affiliated with IUMS. Strategies identified through key-informant interviews were divided into four theme clusters: the health system, the insurer, the healthcare provider, and the healthcare recipient. The Ministry of Health plays a key role in reducing induced demand through the referral system, which aims to promote prevention and health instead of treatment, and thus, reduce medical costs. Strengthening the referral system can limit people’s self-referral to specialized and highly specialized care. This reduces the provision of unnecessary services. Riahi et al. (18). identified the declining influence of referral and family medicine programs since the implementation of the Health Transformation Plan (HTP) as a key factor in the induced demand for health care in Iran.
One of the important strategies in this field is the development, implementation, and evaluation of policies to prevent induced demand for medication administration. Increasing the price of medical services may not be an appropriate way to prevent induced demand for prescribed medications. Dusansky's study showed that the increase in the price of medical services reduces the demand for healthcare and increases the demand for insurance. This increases the demand for healthcare (19). A study in India demonstrated that government financial support has led to the creation of induced demand for health (20).
A major obstacle is the lack of shared treatment protocols among physicians, which makes monitoring much more complicated. Clinical guidelines are not widely used in Iran’s health system as there are no rules or structures compelling physicians to follow them. Developing clinical guidelines is effective in reducing unnecessary services (16, 21). When the standard of care is unclear or the clinical values are not correctly defined, doctors are motivated to direct their patients to more expensive services. Bickerdyke et al. (7) conducted a study in the field of supplier-induced demand in 2002. The results showed that the more complex and uncertain a service is, the greater the potential possibility of induced demand would be. Weakness of laws, improper implementation of health system policies, and scientific ability also lead to induced demand. Acctually, one of the major obstacles is the lack of common treatment protocols among doctors, which has caused the complexity of monitoring. Clinical guidelines are not used much in the country's health system. In fact, there are no necessary laws and proper structures to provide clinical guidelines in the health system. For this reason, doctors are not required to follow clinical guidelines (7).
Insurance companies can also play a more effective role in curtailing induced demand. From the perspective of the interviewees, insurer-related strategies for the reduction of induced demand included expanding the monitoring role of insurance companies, setting insurance premiums based on the ability to pay, charging deductibles, mandatory universal insurance coverage, following strategic purchasing guidelines, delegating coverage of services to private insurance companies, setting premium limits, conducting applied research and drawing on past experiences. Induced demand leads to uncontrollable costs and additional financial burdens for insurance companies. This could increase their debt to hospitals and other actors within the health system, which along with limited resources, will prevent them from covering the growing demand for healthcare. In some cases, debt forces insurance companies to cancel a portion of their contracts. For example, one study found that there is a higher inducement of unnecessary services when insurance companies do not effectively monitor and control their payments and do not hold healthcare providers accountable based on established standards (22).
Monitoring by insurance companies is very limited and inconsequential, and is mainly focused on the quantity of covered services. This has created a vacuum in the monitoring of non-covered services which are not effectively filled by any other actor within the health system. Moreover, this limited monitoring by insurance companies occurs after the provision of services to patients, which is a major barrier to lifelong monitoring. Insurers tend to follow physicians and do not investigate whether the services provided have been necessary. Bickerdyke et al. (7) argue that the design of public or private insurance in most Organization for Economic Cooperation and Development (OECD) countries provides patients with little incentive to restrain their demand for medical services. This has created a fertile ground for induced demand. Similarly, Ferguson shows that insurance coverage increases demand for visits. Since most people get coverage for drugs and medical services through the workplace, allowing private insurance companies to cover unlisted services will lead to adverse distributive outcomes (23).
Research has shown that supplemental insurance can increase the use of medical services (24, 25). A study in 2001 revealed that induced demand greatly affects health insurance markets (26). For example, Mahbubi et al. (11) stated that supplemental insurance coverage for war veterans resulted in the provision of a wide range of unnecessary services. These findings further highlight the importance of expanding the monitoring role of insurance companies.
Healthcare provider is another key contributor to induced demand. According to the interviewees, one way of reducing induced demand is through lifelong learning to ensure that physicians are keeping up with the latest advances in medicine. For example, In a study by Abdoli et al. (27), patients are more likely to choose a low-cost treatment option if they receive the right information. A 2018 study found that periodic training of physicians can help prevent unnecessary prescriptions of antibiotics (28). Appropriate recruitment and training of medical and paramedical professionals can be effective in controlling induced demand. In what he termed the ‘availability effect’, Pauly (1980) argued that an increase in the number of physicians relative to the population, causes the physicians’ income to decrease. This provided incentives for inducing more healthcare utilization, that is, healthcare supply creates its own demand (29).
Decision-making by the highest-ranked individual in the medical team and physicians' accountability was another strategy identified by the participants. Nyman identified pre-authorization from the insurer and second opinions as factors in reducing induced demand (30). Changing attitudes in insurance use can also be effective against induced demand. Some physicians may induce demand for income and interest from insurance companies. A 1999 study in the U.S. showed that managed care can reduce unnecessary tests and prescriptions (31).
Finally, the healthcare recipient plays a key role in induced demand. The interviewees believed that social capital development, educating and changing the attitudes of the public, raising awareness among healthcare recipients, and promoting the use of the referral system instead of self-referral to specialty care are effective strategies for reducing induced demand. Doctors' visits for simple problems are a major contributor to induced demand. Sometimes patients visit a doctor with no specific cause, which could encourage inducement of demand. For example, Barigozzi and Levaggi studied the strategic interaction between patients and physicians and found that demand for healthcare is largely dependent upon patient knowledge and understanding of their condition and their choice of treatment (32). Another study in 2005 showed that the level of knowledge and awareness among the public is a key factor in induced demand (4). In addition, unnecessary requests made by the patient can encourage demand inducement. Some patients expect a long list of drugs in their prescriptions. For example, Mahbubi et al. (11) showed that many patients make requests about the type and quantity of drugs. Bickerdyke et al. (7) stated that rising expectations on the part of patients contribute to increases in the rate of usage of medical services. Therefore, it is imperative to educate the public and limit the availability of healthcare services.
One of the limitations of this study was the difficulty in engaging key informants for interviews. This limitation was largely addressed through communication and ongoing follow-up by researchers and attempts to explain the implications of their studies. Overall, Within the structure of this research and the composition of participants chosen for interviews, the results can be generalized to all university hospitals for policy-making at the macro level. However, case studies are desired to achieve a broader aspect of the issue of induced
demand using insights from experts in various fields and professions involved in health.
Conclusion
Overall, regarding the scope of this study and the composition of participants selected for interviews, the results can be generalized to all university hospitals and medical training centers for policymaking at the macro level. However, case studies are required to be more comprehensive and use practical strategies using insights from experts in different fields and occupations involved in healthcare.
Acknowledgments
The authors thank Iran Univerity of Medical Science for data support. This study was supported by Iran Univerity of Medical Science of Iran.
Conflict of interests
The authors declared no conflict of interests.
Authors' contributions
Seyedin H, Afshari M, and Corani Bahador R designed research; Afshari M, Hasanzadeh E, and Radinmanesh M conducted research; Isfahani P, Corani Bahador R analyzed data; and Afshari M, Isfahani P, and Corani Bahador R wrote the paper. Corani Bahador R had primary responsibility for final content. All authors read and approved the final manuscript.
Funding
This study was financially supported by IUMS.
Methods: This was a qualitative study conducted in 2018. The authors conducted in-depth, semi-structured interviews with 20 participants, including IUMS faculty members, physicians, public hospital managers, patients, and researchers with academic and practical experience. Inductive content analysis was used to analyze data. Data analysis was performed in MAXQDA10.
Results: Overall, the authors extracted 24 subthemes from the interviews and classified them into the health system, insurer, healthcare provider, and healthcare recipient. They are key factors regarding the induced demand for healthcare in the public hospitals under study.
Conclusion: Reducing induced demand for healthcare requires concerted actions by health policymakers and managers at the level of the health system, insurers, healthcare providers, and healthcare recipients. Therefore, policymakers and managers of the health system should take appropriate measures such as the development of guidelines and protocols by different departments, especially the emergency department, classification (primary, secondary, and tertiary care), and referral system. They expand the monitoring role of insurance companies (transforming the payment system into the global diagnosis-related group) to reduce the induced demand for health.
Keywords: Induced demand, Hospital, Strategy
Introduction
Induced demand is a long-debated topic in the field of health economics. It is defined as the change in the demand for healthcare associated with the discretionary influence of providers, especially physicians, over their patients (3). As a complex and multidimensional phenomenon, induced demand is a major challenge for health systems worldwide. It creates an imbalance between needs and available resources; thus, increasing patients’ share in healthcare costs and Catastrophic Health Expenditure (CHE) (4).
The concept of supplier-induced demand has been addressed in the health economics
literature for 30 years, and it is one of the
controversial topics in this field. Various definitions have been given for supplier-induced demand. For example, induced demand from Pauly's point of view is" a demand which takes advantage of data more than patients regarding health services and provides excessive care with questionable value" (5). Crane also defines induced demand: "inducing the provision, care or sale of unnecessary services to clients of the health system, which is related to the exercise of power by service providers, is termed induced demand" (6).
This type of demand can be in the form of increasing the number of services or changing the services provided to patients. Induced demand for health services can be related to two types of extensive medical services such as consultation and visits or referrals to diagnostic centers (7). The premise of the supplier-induced demand hypothesis is based on the assumption of asymmetric information between the doctor and the patient. A patient does not have enough information to assess the quantity and quality of services provided. Therefore, the doctor acts as a consultant to the patient and provides medical care to her/him. The doctor can have a significant effect on the type and quality of services provided (8). For example, a study in the United States showed that there was a significant relationship between the number of doctors and the price of services, and the number of consultations and visits (9).
Induced demand undermines the efficient allocation of national resources, even when all the costs are paid by patients. This situation can disturb the balance of supply and demand in the healthcare market while imposing additional burdens on the patients. At times, incorrect diagnosis and/or treatment lead to medical complications for care recipients (10, 11) From a health policy perspective, induced demand raises two main concerns. On the one hand, it increases health expenses and puts a burden on government budgets. On the other hand, it affects efficiency, since a higher share of a nation’s resources is devoted to healthcare with few benefits (7). Moreover, induced demand for care could result in a massive economic loss at the national level, especially when the government subsidizes medical services and drugs (12).
Romer and his colleague's studies were the first research on supplier-induced demand, known as Romer's Law in the healthcare market. This law states, “a hospital bed built is a filled bed”. Although this theory has been proposed for demanding hospital services, it can extend to the doctors' services as well (13). The service provider has no motivation to provide services at an optimal level, and providing unnecessary services causes a waste of resources and inefficiency. This is because they impose additional costs on patients to increase income or anything in their interests (14).
The probability of induced demand occurrence and the intensity of its effects can be the result of the interaction of a wide range of factors that can influence patients' behavior (15). Patients can be influential in creating induced demand from health service providers. Factors such as medical history and physical and mental condition can show patients' preferences and values. Patients have unlimited preferences and desires for health services (7). Moreover, systemic factors can also be another cause of induced demand for health services. These factors can facilitate the creation of induced demand in different ways such as increasing profits, increasing sales of services, and marketing (16). Various reasons lead to an induced demand in the healthcare system. Therefore, the purpose of the present
research is to identify strategies for reducing
induced demand regarding healthcare in Iran as a useful step toward efficient management of the health system, cost containment in the health sector, and, eventually, improved quality of care.
Materials and Methods
This qualitative research was conducted in 2018 in hospitals affiliated with the Iran University of Medical Sciences (IUMS). By conducting semi-structured interviews, researchers identified solutions to reduce induced demand in the health system. The researchers arranged the time and place of the interviews with the participants in advance. Before starting interviews, while explaining the study objectives and the confidentiality of the data, participants completed an informed consent form. Then, they were asked for permission to tape-record their conversations. In addition, researchers tried to obtain complete information about their experiences and opinions about the research objectives.This was done by communicating and interacting effectively with the participants and guiding them to the desired topic. Moreover, during the interviews, notes were taken to confirm the correctness of the data. This was done by restating the important points and summarizing the participants' responses. The interviews were conducted individually and as much as possible in a calm environment without the presence of others.
An interview guide was developed based on the objectives of the research and the literature. Three pilot interviews were conducted to optimize the questions, improve the interviewer’s communication skills, and increase the validity of the research. The participants were selected by experts related to the subject. Accordingly, policymakers, managers and doctors, and employees of health and medical organizations, and faculty members of medical sciences universities across the country with at least 3 years of experience in managerial, executive, and scientific activities were included.
Interviewees were selected using purposive and snowball sampling techniques and interviews continued until saturation was reached (20 interviews). Interviews were arranged in advance and at the participants’ workplaces. On average, each interview lasted about 36 minutes (30-45 minutes). Interviewees were coded with the letter “M”. Transcripts were 4 to 10 pages long.
Data analysis was done simultaneously with their collection. Immediately after each interview, the authors typed the recorded conversations. Brown and Clark's (17) six-step thematic analysis method, including understanding the data, identifying primary codes, searching for themes, reviewing themes, defining themes, and preparing a report, was used to analyze the qualitative data of this study. Data analysis was performed in MAXQDA10.
The research team increased the validity and generalizability of the research results. This was done using measures such as sampling with maximum diversity; conducting pilot interviews; long contact with the research environment; spending enough time to conduct interviews; examining the issue from different angles; collecting as much information and evidence as possible, collecting and analyzing documents; comparing the obtained information; sending the findings to a sample of the interviewees and including their additional comments; exchanging opinions with peers and scrutinizing the research environment and the steps of the research. In addition, pilot interviews, careful explanation of the interview procedure, triangulation of the obtained data, and gathering more information and evidence were measures the authors took to ensure objectivity. Ethical considerations included complying with the IUMS ethics code (IR.IUMS.REC 1396.30888), acquiring informed consent, asking permission to record interviews, maintaining confidentiality, and avoiding bias in data collection, analysis, and reporting.
Results
20 faculty members, physicians, public hospital managers, patients, and researchers with academic and practical experience participated in this study (Table 1). 4 themes and 24 subthemes on strategies for the reduction of induced demand for healthcare were extracted from the interviews. The main themes included the health system, the insurer, the healthcare provider, and the healthcare recipient (Table 2).
Theme 1: Strategies related to the health system
The interviewees offered nine strategies related to the health system which could be effective for reducing induced demand for health care: monitoring the role of the health system; health system reform; classification and referral system; conducting health information technology studies for medical equipment imports; tax reform and implementation of a progressive tax system; medical education and medical curriculum reforms; legal reform and specification of the professional responsibilities of physicians; transparency of the basic healthcare package; and prevention-centered instead of treatment-centered perspective. Some of the comments made by the interviewees are as follows:
“Monitoring and investigating should occur in the current situation. The authors have to ensure that the right technologies are imported, and also make sure that they are used correctly. For example, anyone with a knee injury can receive an MRI, but is it really necessary? It depends on the patient. Classification of care in the private sector was excluded from the Fourth Development Plan, and about 250 MRI licenses were issued for Tehran. But the Fifth Development Plan included this classification; wrong licenses were issued and prices went up. This imposed a massive financial burden on the system.” (M1) (monitoring role of the health system)
“The best thing is to sever the financial link between the physician and the patient completely. I mean, the patient doesn’t pay out-of-pocket, and the insurance company covers the costs, especially private insurance companies because public insurance companies don’t really care much about the number of services provided. In a nutshell, there should be no financial link between physicians and patients, and coverage of services should be delegated to private insurance companies.” (M2) {payment system reform)
“Payment reforms can be very helpful; we should have the right price for services.” (M3) (payment system reform)
“First and foremost, we have to adjust the Fee-For-Service (FFS) system, which is currently the dominant payment system in the country. If the share of FFS in the salary is higher, the likelihood of inducing demand increases. In developed countries, FFS constitutes only a small part of a person’s salary to motivate the provision of care. The opposite is true in Iran. FFS makes up a large part of the person’s salary. In order to motivate physicians without encouraging inducement of demand, FFS shouldn’t be greater than their salary.” (M4) (payment system reform)
“We’re a Third World country, so we should have some mechanisms for evaluating the import of certain technologies. When too many MRI machines are imported, owners are more likely to encourage physicians to induce demand for its use. Those mechanisms should provide oversight and prevent this.” (M5) (conducting IT studies regarding health for equipment imports)
“Our tax system should be transparent. It can foster certain behaviors. Our tax system should be linked to our information systems. Some countries implement a progressive tax system for physicians. For example, those earning $100,000 are taxed at a certain rate, those earning $150,000 are taxed at a slightly higher rate, and so on. Sometimes income tax rate reaches 90 %, and the individual has no incentive to provide more services. Progressive tax can be very beneficial in preventing induced demand. Of course, there has to be an oversight to deter physicians from selecting easy cases and rejecting more complex ones.” (M4) (tax reform and implementation of a progressive tax system)
“The next strategy is curriculum reform. General Practitioners (GPs) are capable of performing a lot of tasks. But in Iran, there are GPs who can hardly perform basic tests. If authorities manage to update general practice education programs, they’ll be able to reduce costs significantly, especially at a time when the country is struggling with sanctions and other problems.” (M7) (medical education and medical curriculum reforms)
“There should be transparency in our Basic Health Care package. Priorities should be based on the incidence of diseases and disabilities and the mortality rate. Interventions should be practical; for example, when a healthcare package is to be proposed, it must have a healthcare standard attachment, a clinical guidelines attachment, a health system attachment, and an accreditation system attachment. Ensuring these is a big step toward health system reform.” (M8) (transparency in the Basic Health Care package)
Theme 2: Strategies related to the insurer
Eight strategies related to the insurer were identified by the interviewees: expanding the monitoring role of insurance companies; setting insurance premiums based on the ability to pay; charging deductibles; mandatory universal insurance coverage; following strategic purchasing guidelines; delegating coverage of services to private insurance companies; setting premium limits; and conducting applied research and drawing on past experiences. Some of the comments made by the interviewees are as follows:
“The health system and the insurance system must have strict regulations on monitoring, and conflicts of interest must be managed.” (M9) (expanding the monitoring role of insurance companies)
“The problem is that paragraph B of article 38 in the fifth development plan, and paragraph A of article 70 in the sixth development plan, which highlights mandatory universal health insurance coverage, haven’t been implemented yet. This is one of the main pillars of the health system. These laws can clarify our policies and inform us about vulnerable people who must be covered, people who must contribute to national insurance, and people who must pay both premium and progressive tax. Then, we can talk about the financial relationship between physicians and patients. It all comes down to the paying ability of our insurance companies and competition in the market. Many countries have reduced the financial relationship between physicians and patients to zero. In many countries such as Thailand and Turkey, a physician is the team supervisor. Based on our healthcare resources, government assistance, and patients’ deductibles, we can determine the extent of support and coverage that can be provided. We must take action to provide social support for patients and make sure that they don’t suffer high medical expenditures.” (M10) (setting insurance premiums based on the ability to pay)
“Insurance companies are the biggest stakeholders and must make sure that this notion is understood within the health system. They must recognize that induced demand will lead to a budget deficit and bankruptcy, just like the Social Security Insurance Organization which has declared bankruptcy. This organization doesn’t charge any deductibles on its affiliated hospitals, which has resulted in a great deal of induced demand. There are cases of multiple revisits in one month with the same diagnosis and the same drugs, which are sometimes not even used.” (M11) (charging deductibles)
“If insurance companies play an active role and act according to strategic purchasing guidelines, induced demand can be controlled to a large extent, which is especially important now that lack of resources is more strongly felt more than ever.” (M12) (following strategic purchasing guidelines)
Theme 3: Strategies related to the healthcare provider
Five effective strategies related to the healthcare provider were identified by the interviewees: severing direct links between companies and physicians; establishing a team within the hospital to monitor induced demands; lifelong learning; medical decision-making by the highest-ranked individual in a medical team; and physician's accountability. Some of the comments made by the interviewees are as follows:
“Preventing direct links between companies and physicians can be very advantageous.” (M13) (severing direct links between companies and physicians)
“A strong team or committee can be established within the hospital, consisting of several key individuals such as the CEO and managers of different departments to address the unnecessary services that are provided and come up with mechanisms to monitor and prevent it.” (M14) (establishing a team within the hospital to monitor induced demands)
“Physicians who graduate from medical schools no longer receive education and many of them continue working based on the knowledge acquired in the past. Despite the fast changes and advances in medical science, they keep relying on outdated information. Effectiveness of some treatments can be calculated using software, but they don’t receive training and are not updated; therefore, induced demand still exists.” (M15) (lifelong learning)
“Clinical decisions should be made by the highest-ranked physician in the medical team to increase physicians’ confidence and allow them to work without being unnecessarily concerned about legal issues.” (M16) (medical decision-making by the highest-ranked individual in a medical team)
Theme 4: Strategies related to the healthcare recipient
According to the interviewees, there are four effective strategies related to the healthcare recipient which can help reduce induced demand. They include social capital development, educating and changing the attitudes of the public, raising awareness among healthcare recipients, and promoting the use of the referral system instead of self-referral to specialty care. Some of the comments made by the interviewees are as follows:
“The issue of social capital is very important; it influences the behavior of healthcare consumers, the behavior of healthcare providers, and the behavior of social mechanisms. This requires strengthening certain things such as associations and seminars.” (M17) (social capital development)
“We must embed public health into culture through mass media instead of encouraging unhealthy lifestyles. These issues can also be promoted through digital media or by distributing pamphlets in organizations, schools, universities, etc.” (M18) (educating and changing attitudes of the public)
“Another way is to raise awareness among healthcare recipients about induced demand and encourage them to consult with informed individuals.” (M19) (raising awareness among healthcare recipients)
Table 1. Demographic characteristics of the interviewees
| Variable | Frequency | Percentage | |
| Gender | Female | 4 | 20 |
| Male | 16 | 80 | |
| Age | < 30 yrs. | 0 | 0 |
| 31-40 yrs. | 4 | 20 | |
| 41-50 yrs. | 14 | 70 | |
| > 50 yrs. | 2 | 10 | |
| Marital Status | Single | 0 | 0 |
| Married | 20 | 100 | |
| Experience | < 10 yrs. | 4 | 20 |
| 10-20 yrs. | 8 | 40 | |
| 21-30 yrs. | 6 | 30 | |
| > 30 yrs. | 2 | 10 | |
| Education | Bachelor of medicine | 0 | 0 |
| Masters of sciences | 4 | 20 | |
| Medical Doctor (MD) | 8 | 40 | |
| MD with Specialization | 8 | 40 | |
| Employment | Official | 17 | 85 |
| Contractual | 3 | 15 |
Discussion
One of the important strategies in this field is the development, implementation, and evaluation of policies to prevent induced demand for medication administration. Increasing the price of medical services may not be an appropriate way to prevent induced demand for prescribed medications. Dusansky's study showed that the increase in the price of medical services reduces the demand for healthcare and increases the demand for insurance. This increases the demand for healthcare (19). A study in India demonstrated that government financial support has led to the creation of induced demand for health (20).
A major obstacle is the lack of shared treatment protocols among physicians, which makes monitoring much more complicated. Clinical guidelines are not widely used in Iran’s health system as there are no rules or structures compelling physicians to follow them. Developing clinical guidelines is effective in reducing unnecessary services (16, 21). When the standard of care is unclear or the clinical values are not correctly defined, doctors are motivated to direct their patients to more expensive services. Bickerdyke et al. (7) conducted a study in the field of supplier-induced demand in 2002. The results showed that the more complex and uncertain a service is, the greater the potential possibility of induced demand would be. Weakness of laws, improper implementation of health system policies, and scientific ability also lead to induced demand. Acctually, one of the major obstacles is the lack of common treatment protocols among doctors, which has caused the complexity of monitoring. Clinical guidelines are not used much in the country's health system. In fact, there are no necessary laws and proper structures to provide clinical guidelines in the health system. For this reason, doctors are not required to follow clinical guidelines (7).
Insurance companies can also play a more effective role in curtailing induced demand. From the perspective of the interviewees, insurer-related strategies for the reduction of induced demand included expanding the monitoring role of insurance companies, setting insurance premiums based on the ability to pay, charging deductibles, mandatory universal insurance coverage, following strategic purchasing guidelines, delegating coverage of services to private insurance companies, setting premium limits, conducting applied research and drawing on past experiences. Induced demand leads to uncontrollable costs and additional financial burdens for insurance companies. This could increase their debt to hospitals and other actors within the health system, which along with limited resources, will prevent them from covering the growing demand for healthcare. In some cases, debt forces insurance companies to cancel a portion of their contracts. For example, one study found that there is a higher inducement of unnecessary services when insurance companies do not effectively monitor and control their payments and do not hold healthcare providers accountable based on established standards (22).
Monitoring by insurance companies is very limited and inconsequential, and is mainly focused on the quantity of covered services. This has created a vacuum in the monitoring of non-covered services which are not effectively filled by any other actor within the health system. Moreover, this limited monitoring by insurance companies occurs after the provision of services to patients, which is a major barrier to lifelong monitoring. Insurers tend to follow physicians and do not investigate whether the services provided have been necessary. Bickerdyke et al. (7) argue that the design of public or private insurance in most Organization for Economic Cooperation and Development (OECD) countries provides patients with little incentive to restrain their demand for medical services. This has created a fertile ground for induced demand. Similarly, Ferguson shows that insurance coverage increases demand for visits. Since most people get coverage for drugs and medical services through the workplace, allowing private insurance companies to cover unlisted services will lead to adverse distributive outcomes (23).
Research has shown that supplemental insurance can increase the use of medical services (24, 25). A study in 2001 revealed that induced demand greatly affects health insurance markets (26). For example, Mahbubi et al. (11) stated that supplemental insurance coverage for war veterans resulted in the provision of a wide range of unnecessary services. These findings further highlight the importance of expanding the monitoring role of insurance companies.
Healthcare provider is another key contributor to induced demand. According to the interviewees, one way of reducing induced demand is through lifelong learning to ensure that physicians are keeping up with the latest advances in medicine. For example, In a study by Abdoli et al. (27), patients are more likely to choose a low-cost treatment option if they receive the right information. A 2018 study found that periodic training of physicians can help prevent unnecessary prescriptions of antibiotics (28). Appropriate recruitment and training of medical and paramedical professionals can be effective in controlling induced demand. In what he termed the ‘availability effect’, Pauly (1980) argued that an increase in the number of physicians relative to the population, causes the physicians’ income to decrease. This provided incentives for inducing more healthcare utilization, that is, healthcare supply creates its own demand (29).
Decision-making by the highest-ranked individual in the medical team and physicians' accountability was another strategy identified by the participants. Nyman identified pre-authorization from the insurer and second opinions as factors in reducing induced demand (30). Changing attitudes in insurance use can also be effective against induced demand. Some physicians may induce demand for income and interest from insurance companies. A 1999 study in the U.S. showed that managed care can reduce unnecessary tests and prescriptions (31).
Finally, the healthcare recipient plays a key role in induced demand. The interviewees believed that social capital development, educating and changing the attitudes of the public, raising awareness among healthcare recipients, and promoting the use of the referral system instead of self-referral to specialty care are effective strategies for reducing induced demand. Doctors' visits for simple problems are a major contributor to induced demand. Sometimes patients visit a doctor with no specific cause, which could encourage inducement of demand. For example, Barigozzi and Levaggi studied the strategic interaction between patients and physicians and found that demand for healthcare is largely dependent upon patient knowledge and understanding of their condition and their choice of treatment (32). Another study in 2005 showed that the level of knowledge and awareness among the public is a key factor in induced demand (4). In addition, unnecessary requests made by the patient can encourage demand inducement. Some patients expect a long list of drugs in their prescriptions. For example, Mahbubi et al. (11) showed that many patients make requests about the type and quantity of drugs. Bickerdyke et al. (7) stated that rising expectations on the part of patients contribute to increases in the rate of usage of medical services. Therefore, it is imperative to educate the public and limit the availability of healthcare services.
One of the limitations of this study was the difficulty in engaging key informants for interviews. This limitation was largely addressed through communication and ongoing follow-up by researchers and attempts to explain the implications of their studies. Overall, Within the structure of this research and the composition of participants chosen for interviews, the results can be generalized to all university hospitals for policy-making at the macro level. However, case studies are desired to achieve a broader aspect of the issue of induced
demand using insights from experts in various fields and professions involved in health.
Conclusion
Overall, regarding the scope of this study and the composition of participants selected for interviews, the results can be generalized to all university hospitals and medical training centers for policymaking at the macro level. However, case studies are required to be more comprehensive and use practical strategies using insights from experts in different fields and occupations involved in healthcare.
Acknowledgments
The authors thank Iran Univerity of Medical Science for data support. This study was supported by Iran Univerity of Medical Science of Iran.
Conflict of interests
The authors declared no conflict of interests.
Authors' contributions
Seyedin H, Afshari M, and Corani Bahador R designed research; Afshari M, Hasanzadeh E, and Radinmanesh M conducted research; Isfahani P, Corani Bahador R analyzed data; and Afshari M, Isfahani P, and Corani Bahador R wrote the paper. Corani Bahador R had primary responsibility for final content. All authors read and approved the final manuscript.
Funding
This study was financially supported by IUMS.
Type of Study: Original article |
Subject:
Health Economics
Received: 2022/07/20 | Accepted: 2022/10/26 | Published: 2022/12/31
Received: 2022/07/20 | Accepted: 2022/10/26 | Published: 2022/12/31
References
1. Shepherd D, Hodgkin D, & Anthony Y. Analysis of hospital costs: A manual for managers. geneva: World Health Organization; 2002.
2. Maizel S, Passarelli S, Pillari GD. The financial crisis facing America’s hospital industry: Part I. American Bankruptcy Institute Journal. 2007.
3. Seyedin H, Afshari M, Isfahani P, Hasanzadeh E, Radinmanesh M, Bahador RC. The main factors of supplier-induced demand in health care: A qualitative study. Journal of Education and Health Promotion. 2021; 10: 49. [DOI: 10.4103/jehp.jehp_68_20]
4. Abdoli, G. Induce demand: Theory of information asymmetry between patients and doctors. Iranian Journal of Health Economics Research. 2005; 68: 91-114. [In Persian]
5. Pauly MV. Doctors and Their Workshops: Economic Models of Physician Behavior. University of Chicago Press: University of Chicago Press; 2009.
6. Crane ThS. The problem of physician self-referral under the medicare and medicaid anti-kickback statute. The Hanlester Network Case and the Safe Harbor Regulation. Journal of the American Medical Association. 1992; 68(1): 85-91. [DOI: 10.1001/jama.1992.03490010087035]
7. Bickerdyke I, Dolamore R, Monday I, Preston R. Supplier-induced demand for medical services. Canberra: Productivity Commission Staff Working Paper; 2002.
8. Grytten J, Sørensen R. Type of contract and supplier-induced demand for primary physicians in Norway. Journal of Health Economics. 2001; 20(3): 379-93. [DOI: 10.1016/s0167-6296(00)00087-4]
9. Wilensky GR, Rossiter LF. The relative importance of physician-induced demand in the demand for medical care. The Milbank Memorial Fund Quarterly. 1983; 61(2): 252-77. [DOI: 10.2307/3349907]
10. Izumida N, Urushi H, Nakanishi S. An empirical study of the physician-induced demand hypothesis: The cost function approach to medical expenditure of the elderly in Japan. Review of Population and Social Policy. 1999; 8: 11-25.
11. Mahbubi M, Ojaghi S, Ghiasi M, Afkar, A. Supplemental insurance and induced demand in chemical warfare veterans. Iranian Journal of Journal of Military and Veterans’ Health. 2010; 2(4): 18-22. [In Persian]
12. Ansari B, Hosseini SM, Bahadori M. Deter-minants of reduction of induced demand in selected hospitals affiliated with IUMS: A qualitative study from the provider’s perspective. Urmia Nursing and Midwifery Faculty Journal. 2018; 16(6): 389-402. [In Persian]
13. Roemer MI. Bed supply and hospital utilization: A natural experiment. Hospitals. 1961; 35: 36-42.
14. Bajari P, Hong H, Khwaja A. Moral hazard, adverse selection and health expenditures: A semiparametric analysis. National Bureau of Economic Research. 2006.
15. Wanderling D, Groen R, Belak N. Textbook of health economics. Trans. Tofighi S, Ahmadkiadeliri A,Haghparast H. Tehran, Iran: Vajepardazan; 2010. [In Persian]
16. Keyvanara M, Karimi S, Khorasani E, Jafarian Jazi M. Are health institutions involved in health care induced demand? (a qualitative study). Payavard Salamat. 2014; 8(4): 280-93. [In Persian]
17. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006; 3(2): 77-101.
18. Riahi, M., Taleghani, Y. M., Salehiniya, H., & Vejdani, M. Induced demand: A challenge on the way of Iran’s health transformation plan. Journal of Pharmaceutical, Biological and Chemical Sciences. 2016; 7(5): 1827-35.
19. Dusansky R, Koç Ç. Implications of the interaction between insurance choice and medical care demand. J Risk Insur. 2010; 77: 129-44. [DOI: 10.1111/j.1539-6975.2009.01335.x]
20. Bogg L, Diwan V, Vora KS, DeCosta A. Impact of alternative maternal demandside financial support programs in India on the Caesarean section rates: Indications of supplier-induced demand. Matern Child Health J. 2016; 20(1): 11–5. [DOI: 10.1007/s10995-015-1810-2]
21. Akhavan Behbahani A, Esmaili I. Supplier-induced demand (SID) for medical services by Iranian physicians (policymaking and controlling). Majlis & Rahbord, 2019; 25(96): 321-41. [In Persian]
22. Dranove D. Health care markets, regulators, and certifiers. Handbook of Health Economics, 2011; 2: 639-90.
23. Ferguson BS, Crawford A. Supplier–induced demand: A disequilibrium test. Applied Economics. 1989; 21(5): 597-610. [DOI: 10.1080/758524893]
24. Seyedin H, Afshari M, Isfahani P, Rakhshan A, Hasanzadeh E, Taherimirghaed M. Main Factors leading to supplier-induced demand in Iran: A comprehensive review. Health Scope. 2020; 9(2): e96366. [DOI: 10.5812/jhealthscope.96366]
25. Hickson GB, Altemeier WA., Perrin JM. Physician reimbursement by salary or fee-for-service: Effect on physician practice behavior in a randomized prospective study. Pediatrics, 1987; 80(3): 344-450.
26. Fabbri D, Monfardini Ch. Demand induction with a discrete distribution of patients. First Edition. Italy, Bologna: University of Bologna; 2001.
27. Abdoli G, Varharami V. The role of asymmetric information in induced demands: A case study of medical services. Iranian Journal of Health Administration. 2011; 14(43): 37-42. [In Persian]
28. Barari M, Afrasiabian Sh, Mohsenpour B, Hajibagheri K, Sheikhesmaili F. Evaluation of appropriate antibiotic administration by general practitioners at the emergency department of a teaching hospital in Sanandaj, Iran. Scientific Journal of Kurdistan University of Medical Sciences. 2018; 23(3): 67-72. [In Persian]
29. Pauly M. Doctors and Their Workshops: Economic Models of Physician Behavior. First Edition. Chicago: University of Chicago Press; 1980.
30. Nyman JA. The economics of moral hazard revisited. Journal of Health Economics. 1999; 18(6): 811-24. [DOI: 10.1016/s0167-6296(99)00015-6]
31. Marcus, D. Coordinating care in an uncoordinated health system: The development and implementation of coordinated care trials in Australia. Department of the Parliamentary Library. 1999.
32. Barigozzi F, Levaggi R. Emotions in physi-cian agency. Health Policy, 2008; 88(1): 1-14. [DOI: 10.1016/j.healthpol.2008.03.005]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
