

Volume 6, Issue 4 (10-2022)
EBHPME 2022, 6(4): 262-272 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Izadi H. The Effects of Policy Change Regarding Health Expenditures on Households Behavior. EBHPME 2022; 6 (4) :262-272
URL: http://jebhpme.ssu.ac.ir/article-1-409-en.html
URL: http://jebhpme.ssu.ac.ir/article-1-409-en.html


Department of Economics, Faculty of Management and Humanities, Chabahar Maritime University, Chabahar, Iran , izadi@cmu.ac.ir
Full-Text [PDF 891 kb]
(477 Downloads)
| Abstract (HTML) (1123 Views)
Full-Text: (315 Views)
Background: In order to assess households' socioeconomic level in society, policymakers and government planners pay close attention to families' access to health services. They calculate the percentage of a household's bundle of consumer goods and services. In this regard, the current study examines and analyzes the household's behavior as a result of the government's policies in changing and determining the share of the household's health expenses from its total consumption expenses. This is to ensure that society is kept at a minimum level of health.
Methods: In order to accurately execute health policies and change household behavior, this research studies the share and access of Iranian households to health products and services. The author used a Dynamic Stochastic General Equilibrium model through quarterly data from 1997 to 2020.
Results: Findings show that as this share increased, other items' consumption and utility decreased, which ultimately led to a fall in society's total utility according to the definition that utility is a term used as a measure of pleasure or happiness resulting from consuming goods and services.
Conclusion: The government and policymakers need to bear some of health expenditures and provide financial support to households until it reaches the desired level. This is to prevent a significant decrease in the level of total utility in society. This decrease is brought on by people's dissatisfaction with spending a larger portion of their expenses on health goods and services.
Keywords: Health expenditures, Households’ behavior, Policy, Changes
Health is one of the key prerequisites for the utility and social welfare systems. People are compelled to utilize health services and even pay for them. This is in addition to having a healthy lifestyle. Demand for services and the willingness to utilize them are two connected ideas. From an economic perspective, a person's financial status to use health services is influenced by the cost and value of such services. On the other hand, the connection between the demand and Supply of health services leads to purchasing health services in addition to people's needs (2).
The demand for health and health services is also influenced by several variables, including consumer behavior, socioeconomic status, age distribution, health status, and income and education levels. On the other hand, disease-related economic expenses have increased. They include the price of services to diagnose and treat the illness. In addition, the reduction in income brought on by the sick person's decreased productivity and working ability also causes these costs to rise. This problem raises the likelihood of a family's financial crisis. As a result, health economics is increasingly concerned with health expenditures and the factors influencing them (3).
Based on out-of-pocket payments and advance payments, experts classified household health expendituresWhen patients say they are paying out of pocket, they mean they pay for services themselves. In reality, advance payments are contributions made through general tax, bill tax, and compulsory and voluntary insurance (4).
The significance of this issue can be addressed in two parts: on the one hand, the high share of household expenditures, which results in unequitable participation in payment. This increases the percentage of households facing disastrous health expenditures. On the other hand, there had been a rapid growth in health costs since the 1960s. This is primarily caused by various factors such as population growth, changes in people's expectations, and the tendency to use new and effective treatments (5).
Adequate access of all members of society to health services and products is one of the primary difficulties facing the political and economic authorities of the countries. It should be underlined that the primary determinant of everyone's appropriate access to health care is the means for paying for these products and services. This indicates that if a family cannot afford to pay for health-related products and services, authorities must lower the price of other goods and services to free up money for health-related costs. As a result, people will either stop using other products and services entirely or limit them to below the ideal level. This has drastically declined society's overall well-being, which will be regarded as a major harm. Therefore, it is crucial to identify how households pick and pay for the health products and services they need (6).
Economists in developed countries employed large-scale structural macroeconomic models to examine the consequences of macroeconomic policies between the 1960s and the late 1970s. However, the academic community and specialized organizations and institutions adopted these models less over time due to Lucas's critiques (Robert Lucas argues that it is naive to predict the effects of a change in economic policy entirely based on relationships observed in historical data, especially highly aggregated historical data. More formally, it states that the decision rules of Keynesian models—such as the consumption function—cannot be considered structural in the sense of being invariant concerning changes in government policy variables). Dynamic Stochastic General Equilibrium (DSGE) models a new generation of methods created to address this set of issues, which are extensively employed by decision-makers. Along with the fact that Lucas's critique does not apply to these models, one of their hallmarks is that they are built on the principles of microeconomics (7, 8).
The real business school first employed DSGE models as a tool for macroeconomic research, and these models eventually found their way into actual business cycle models. In contrast to modern ones, the classic Keynesian models were mostly utilized for qualitative research and were based on static models with little indication of the dynamic optimization issues faced by households and businesses. This problem is the catalyst for merging these two theories. In the late 1990s, new neoclassical synthesis models or new Keynesian models (New Keynesian economics is a school of macroeconomics that strives to provide microeconomic foundations for Keynesian economics. It developed partly as a response to criticisms of Keynesian macroeconomics by adherents of new classical macroeconomics) resulted from this blending (9).
In a dynamic stochastic general equilibrium model, analysis of aggregate supply and demand sectors requires the study of the consumption and production units of the economy. Therefore, deriving equations related to aggregate demand requires the analysis of consumer behavior. Moreover, equations related to the aggregate supply require the analysis of the behavior of the economic enterprise. In these models, equations are extracted based on the principles of microeconomics, and then, the behavior of each unit is determined by optimizing its purposes. Therefore, author can determine the behavior of households by solving the problem of maximization of the utility function, and the maximization of the profit function will define the firms' behavior (10).
This paper tries to investigate the effects of policy change regarding health expenditures on households’ behavior. This was done using the DSGE model for Iran's economy. By defining the utility functions for households, this research model separates households' utility and consumption functions and has the utility of total goods, the utility of health goods, the utility of other goods, consumption of total goods, consumption of health goods, and consumption of other goods sections. In the following, recent papers are using this type of utility and consumption function and modeling. They include Grossman (11), Gerdham et al. (12), Getzen (13), Guisan et al. (14), Matsaganis et al. (15), Mullahy (16), Wang (17), Malik et al. (18), Lee et al. (19) and Brown et al. (20).
Governments and policymakers have made plans and taken action to overcome the barriers. They may cause disruptions or move towards a goal other than the one determined to increase the welfare and health of society. These plans and actions consider variation in households' access to health services as well as their non-uniform share of these services regarding the total consumption expenditure of households in the country. The way the government operates in this area has a significant impact. This is crucial, even if the change in the proportion of health services in household costs is mostly tied to social development and people's knowledge. As a result, this study considers how changes in the percentage of healthcare products and services regarding their desirability function have affected the government's policies on household behavior.
This paper builded a model with the different utilities, considering the different effects of health expenditures on the behavior of households on economic models. It aimed to examine business cycles in the Iranian economy resulting from this issue and their effects on the behavior of macroeconomic variables. The author obtained quarterly data from 1997 to 2020 from the statistical center of Iran, the central bank, and domestic, international and World Bank financial statistics.
Materials and Methods
This research tries to investigate household behaviour using time series data, library research, data analysis, and the DSGE method for Iran's economy in the field of health. For this aim, quarterly data from 1997 to 2020 has been obtained and used from the statistical center of Iran, the central bank, and domestic, international and world bank financial statistics and data. In a dynamic stochastic general equilibrium model, the analysis and extraction of the consumption and production of the economic units and the equations related to this section are essential to the analysis of the behavior of the economic agents. Therefore, the households determined the problem of maximization of the utility function and profit function of firms. This research designed and implemented a model using Smets et al. (21) and Izadi (22) models, and applied the DSGE method. This is popular among many identical households preferring discount factor. It depends on their labor (workforce) and consumption levels described by the below utility functions. This paper used economic studies to build a model for studying household health expenditures and described the variables and behavior of households. The government imposes labor and capital income taxes and operates with a balanced budget. Equations are defined as follows:

 is the consumption of total goods,
is the consumption of total goods, .PNG) is the consumption of health care services,
is the consumption of health care services,  is the consumption of other goods,
is the consumption of other goods, θ  is a labor of households,
is a labor of households,  indicates the interest rate,
indicates the interest rate,  domestic output,
domestic output,  , gross investment,
, gross investment,  , physical capital,
, physical capital, δ  , the labor-augmented technical progress with an AR (1) process as the productivity shock,
, the labor-augmented technical progress with an AR (1) process as the productivity shock, g t .PNG) , use of total goods,
, use of total goods,  , use of health care services,
, use of health care services,  using other products,
using other products,  , wages, and
, wages, and  is the government expenditure.
is the government expenditure.
Results
Researcher examine health expenditures from various aspects. This is because of the important role of health expenditures in society, the use of health services, and creation a favorable environment for households in any country. Parameters and the Bayesian method have been used by equations of the previous section and the DSGE model according to the structure of Iran's economy.
Based on the literature on economy models, to solve and simulate the pattern, the parameter values have been replaced by the calibration method in the Dynare software (Matlab). The research model used the values listed in Table 1. Tables 2 and 3 illustrate the impacts of changes regarding the proportion of household health expenditure with different values. Then, the mean, standard deviation, variance and skewness of the variables were determined. These tables indicate the increase and decrease of the parameter
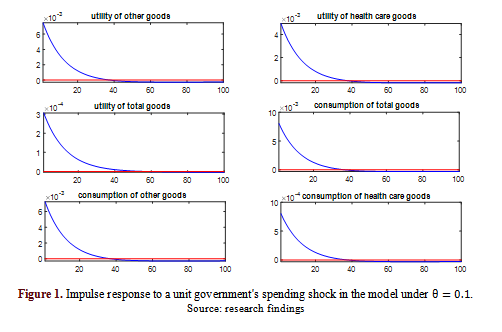
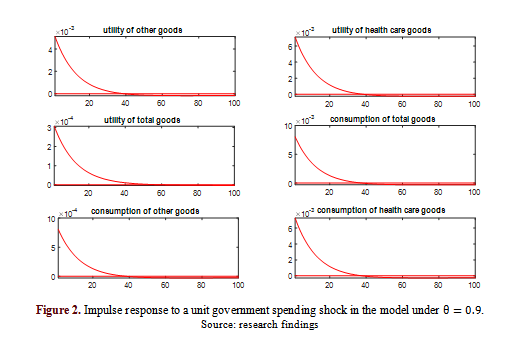
Figures 1 and 2 show the impulse response function of the government's spending shock concerning changes in household health spending
Source: research findings
Source: research findings
Discussion
Five sources are available to the government for the financing health system: households, public expenditure, social security funds, commercial insurances, and entities like charities and non-governmental organizations. Households in developing countries bear the primary financial burden of using the health system; as a result, consumers directly cover the health costs. Of course, this payment system is unfaire, and people's use of health services is determined by their financial situation and capacity to pay, not by their needs or the state of their physical and mental health. Thus, governments are seeking more equitable approaches. Accordingly, the author of this study was seeking efficient laws governing people's access to health-related products and services in Iran. This research aimed to improve the negative state of the household's health. Over the last three decades, there has been a positive trend in raising society's level of health, reducing epidemics, and raising health indicators.
Based on the tables, certain variables have decreased at low levels of
The results show that the lower the
The results suggest that the lower the
Conclusion
A change in the consumption expenditure of other goods and the family's preferences will result from the implementation of any government policy or a shift in the household's attitude. This increases health expenmditures compared to the total consumption bundle. The key takeaway is that the choice of consumption between commodities and services related to health and other items influences the amount of money spent on health-related goods and services. Therefore, researchers suggest that officials in this field encourage households to use health services. This is done by enhancing health and treatment facilities, or more precisely, raising the standard of health development across the nation, and expanding the availability of health insurance services. Give specific income to households with more members or lower incomes to avoid burdening them with large health expenditures, which will cause them to utilize these goods and services less. Additionally, various health facilities, organizations, and laws requiring universal insurance coverage may make it easier for households to receive services.
This study examines the effects of policy change on health expenditures of household behavior using the DSGE model. The reduction of total health expenditure has led to an increase in the consumption expenditure of other goods. This increases the household consumption and the welfare of society. The results of this research and modeling indicate that since the family has little tendency to spend a larger share of its total consumption expenditure on health services, an increase in health expenditure causes the household to reduce the consumption of other goods and services. As a result, the total utility of goods and services will fall.
On the other hand, the lower the parameter of household health expenditure, the stronger the impact of the shock on the consumption variable and the utility of other goods and services in the model. If the value of this parameter increases, the impact of the shock on the consumption variable and the utility of health goods and services will be stronger, and the impact of this shock will be more severe. The combination and selection of a household's consumption bundle of goods and services can change the results of shocks and behavior of households. Moreover, the health of households and society casts a shadow on their other activities. Any change in health costs should be considered, and government policies should be adjusted in order to improve health services.
Policies regarding the choice of consumption bundle of health services should be modified. This is because it has an impact on the health of family members and overshadows their other activities. Therefore, it is recommended that insurance coverage be expanded, insurance funds and government support for per capita insurance fees be combined, and household purchasing patterns be changed. This increases and facilitates household access to these services. On the other hand, hasty measures that support widespread health privatizations should be avoided.
Considering the existence of urban and rural households in the country, and the difference in household behavior caused by the government's policy, the author suggests that in the future researchers consider the separation of urban and rural households in their modeling and propose executive policies based on that.
Acknowledgments
The outhors would like to thank the anonymous reviewers and editors for their valuable contribution.
Conflict of interests
The author declared no conflict of interests.
Authors' contributions
Izadi HR designed research, conducted research, analyzed data, and wrote the paper. Izadi HR had primary responsibility for the final content. All authors read and approved the final manuscript.
Funding
Non applicable.
Methods: In order to accurately execute health policies and change household behavior, this research studies the share and access of Iranian households to health products and services. The author used a Dynamic Stochastic General Equilibrium model through quarterly data from 1997 to 2020.
Results: Findings show that as this share increased, other items' consumption and utility decreased, which ultimately led to a fall in society's total utility according to the definition that utility is a term used as a measure of pleasure or happiness resulting from consuming goods and services.
Conclusion: The government and policymakers need to bear some of health expenditures and provide financial support to households until it reaches the desired level. This is to prevent a significant decrease in the level of total utility in society. This decrease is brought on by people's dissatisfaction with spending a larger portion of their expenses on health goods and services.
Keywords: Health expenditures, Households’ behavior, Policy, Changes
Introduction
In any country, controlling health costs and funding the health sector is a crucial problem. It is entirely unjust for households to bear the majority of the costs of subsidizing the health system in Iran. One of the key objectives of health authorities is to develop more equitable techniques. This is done by looking at variables influencing Iranian households' decisions to enter the health market and select appropriate health products and services (1). Health is one of the key prerequisites for the utility and social welfare systems. People are compelled to utilize health services and even pay for them. This is in addition to having a healthy lifestyle. Demand for services and the willingness to utilize them are two connected ideas. From an economic perspective, a person's financial status to use health services is influenced by the cost and value of such services. On the other hand, the connection between the demand and Supply of health services leads to purchasing health services in addition to people's needs (2).
The demand for health and health services is also influenced by several variables, including consumer behavior, socioeconomic status, age distribution, health status, and income and education levels. On the other hand, disease-related economic expenses have increased. They include the price of services to diagnose and treat the illness. In addition, the reduction in income brought on by the sick person's decreased productivity and working ability also causes these costs to rise. This problem raises the likelihood of a family's financial crisis. As a result, health economics is increasingly concerned with health expenditures and the factors influencing them (3).
Based on out-of-pocket payments and advance payments, experts classified household health expendituresWhen patients say they are paying out of pocket, they mean they pay for services themselves. In reality, advance payments are contributions made through general tax, bill tax, and compulsory and voluntary insurance (4).
The significance of this issue can be addressed in two parts: on the one hand, the high share of household expenditures, which results in unequitable participation in payment. This increases the percentage of households facing disastrous health expenditures. On the other hand, there had been a rapid growth in health costs since the 1960s. This is primarily caused by various factors such as population growth, changes in people's expectations, and the tendency to use new and effective treatments (5).
Adequate access of all members of society to health services and products is one of the primary difficulties facing the political and economic authorities of the countries. It should be underlined that the primary determinant of everyone's appropriate access to health care is the means for paying for these products and services. This indicates that if a family cannot afford to pay for health-related products and services, authorities must lower the price of other goods and services to free up money for health-related costs. As a result, people will either stop using other products and services entirely or limit them to below the ideal level. This has drastically declined society's overall well-being, which will be regarded as a major harm. Therefore, it is crucial to identify how households pick and pay for the health products and services they need (6).
Economists in developed countries employed large-scale structural macroeconomic models to examine the consequences of macroeconomic policies between the 1960s and the late 1970s. However, the academic community and specialized organizations and institutions adopted these models less over time due to Lucas's critiques (Robert Lucas argues that it is naive to predict the effects of a change in economic policy entirely based on relationships observed in historical data, especially highly aggregated historical data. More formally, it states that the decision rules of Keynesian models—such as the consumption function—cannot be considered structural in the sense of being invariant concerning changes in government policy variables). Dynamic Stochastic General Equilibrium (DSGE) models a new generation of methods created to address this set of issues, which are extensively employed by decision-makers. Along with the fact that Lucas's critique does not apply to these models, one of their hallmarks is that they are built on the principles of microeconomics (7, 8).
The real business school first employed DSGE models as a tool for macroeconomic research, and these models eventually found their way into actual business cycle models. In contrast to modern ones, the classic Keynesian models were mostly utilized for qualitative research and were based on static models with little indication of the dynamic optimization issues faced by households and businesses. This problem is the catalyst for merging these two theories. In the late 1990s, new neoclassical synthesis models or new Keynesian models (New Keynesian economics is a school of macroeconomics that strives to provide microeconomic foundations for Keynesian economics. It developed partly as a response to criticisms of Keynesian macroeconomics by adherents of new classical macroeconomics) resulted from this blending (9).
In a dynamic stochastic general equilibrium model, analysis of aggregate supply and demand sectors requires the study of the consumption and production units of the economy. Therefore, deriving equations related to aggregate demand requires the analysis of consumer behavior. Moreover, equations related to the aggregate supply require the analysis of the behavior of the economic enterprise. In these models, equations are extracted based on the principles of microeconomics, and then, the behavior of each unit is determined by optimizing its purposes. Therefore, author can determine the behavior of households by solving the problem of maximization of the utility function, and the maximization of the profit function will define the firms' behavior (10).
This paper tries to investigate the effects of policy change regarding health expenditures on households’ behavior. This was done using the DSGE model for Iran's economy. By defining the utility functions for households, this research model separates households' utility and consumption functions and has the utility of total goods, the utility of health goods, the utility of other goods, consumption of total goods, consumption of health goods, and consumption of other goods sections. In the following, recent papers are using this type of utility and consumption function and modeling. They include Grossman (11), Gerdham et al. (12), Getzen (13), Guisan et al. (14), Matsaganis et al. (15), Mullahy (16), Wang (17), Malik et al. (18), Lee et al. (19) and Brown et al. (20).
Governments and policymakers have made plans and taken action to overcome the barriers. They may cause disruptions or move towards a goal other than the one determined to increase the welfare and health of society. These plans and actions consider variation in households' access to health services as well as their non-uniform share of these services regarding the total consumption expenditure of households in the country. The way the government operates in this area has a significant impact. This is crucial, even if the change in the proportion of health services in household costs is mostly tied to social development and people's knowledge. As a result, this study considers how changes in the percentage of healthcare products and services regarding their desirability function have affected the government's policies on household behavior.
This paper builded a model with the different utilities, considering the different effects of health expenditures on the behavior of households on economic models. It aimed to examine business cycles in the Iranian economy resulting from this issue and their effects on the behavior of macroeconomic variables. The author obtained quarterly data from 1997 to 2020 from the statistical center of Iran, the central bank, and domestic, international and World Bank financial statistics.
Materials and Methods
This research tries to investigate household behaviour using time series data, library research, data analysis, and the DSGE method for Iran's economy in the field of health. For this aim, quarterly data from 1997 to 2020 has been obtained and used from the statistical center of Iran, the central bank, and domestic, international and world bank financial statistics and data. In a dynamic stochastic general equilibrium model, the analysis and extraction of the consumption and production of the economic units and the equations related to this section are essential to the analysis of the behavior of the economic agents. Therefore, the households determined the problem of maximization of the utility function and profit function of firms. This research designed and implemented a model using Smets et al. (21) and Izadi (22) models, and applied the DSGE method. This is popular among many identical households preferring discount factor. It depends on their labor (workforce) and consumption levels described by the below utility functions. This paper used economic studies to build a model for studying household health expenditures and described the variables and behavior of households. The government imposes labor and capital income taxes and operates with a balanced budget. Equations are defined as follows:
is the consumption of total goods, is the consumption of health care services, is the consumption of other goods, is a labor of households, indicates the interest rate, domestic output, , gross investment, , physical capital, , the labor-augmented technical progress with an AR (1) process as the productivity shock, , use of total goods, , use of health care services, using other products, , wages, and is the government expenditure.Results
Researcher examine health expenditures from various aspects. This is because of the important role of health expenditures in society, the use of health services, and creation a favorable environment for households in any country. Parameters and the Bayesian method have been used by equations of the previous section and the DSGE model according to the structure of Iran's economy.
Based on the literature on economy models, to solve and simulate the pattern, the parameter values have been replaced by the calibration method in the Dynare software (Matlab). The research model used the values listed in Table 1. Tables 2 and 3 illustrate the impacts of changes regarding the proportion of household health expenditure with different values. Then, the mean, standard deviation, variance and skewness of the variables were determined. These tables indicate the increase and decrease of the parameter
Figures 1 and 2 show the impulse response function of the government's spending shock concerning changes in household health spending
Table 1. Calibration parameters
| Source | Value | Description | Parameters |
| (23) | 0.013 | Depreciation rate | |
| (24) | 2.000 | Risk aversion | |
| (22) | 0.440 | Capital share | |
| (24) | 0.995 | Discount factor | |
| (25) | 0.356 | Tax on Capital | |
| (26) | 0.047 | Tax on Labor | |
| (25) | 0.599 | Technology's shock persistence | |
| (26) | 0.016 | Technology's shock Std.Dev. | |
| (27) | 0.929 | Government's spending shock persistence | |
| (22) | 0.075 | Government's spending shock Std.Dev. | |
| Researcher's calculations | 0.125 | Government expenditure | G/y |
Table 2. Moments of simulated variables under the values
| Variable | Mean | Std. Dev. | Variance | Skewness |
| Utility of total goods | 0.001034 | 0.004942 | 0.000024 | - 0.054360 |
| Utility of health goods | 0.019523 | 0.020082 | 0.000403 | - 0.286343 |
| Utility of other goods | 0.029532 | 0.029156 | 0.000850 | - 0.297781 |
| Consumption of total goods | 17.893250 | 0.029524 | 0.000872 | - 0.315673 |
| Consumption of health goods | 0.161328 | 0.002952 | 0.000009 | - 0.315673 |
| Consumption of other goods | 0.981775 | 0.026571 | 0.000706 | - 0.315673 |
Table 3. Moments of simulated variables under the values
| Variable | Mean | Std. Dev. | Variance | Skewness |
| Utility of total goods | 0.001042 | 0.004938 | 0.000024 | - 0.053802 |
| Utility of health goods | 0.028295 | 0.027803 | 0.000773 | - 0.292797 |
| Utility of other goods | 0.020377 | 0.020691 | 0.000428 | - 0.283686 |
| Consumption of total goods | 17.851480 | 0.029469 | 0.000868 | - 0.311940 |
| Consumption of health goods | 1.029386 | 0.026522 | 0.000703 | - 0.311940 |
| Consumption of other goods | 0.155993 | 0.002947 | 0.000009 | - 0.311940 |
Discussion
Five sources are available to the government for the financing health system: households, public expenditure, social security funds, commercial insurances, and entities like charities and non-governmental organizations. Households in developing countries bear the primary financial burden of using the health system; as a result, consumers directly cover the health costs. Of course, this payment system is unfaire, and people's use of health services is determined by their financial situation and capacity to pay, not by their needs or the state of their physical and mental health. Thus, governments are seeking more equitable approaches. Accordingly, the author of this study was seeking efficient laws governing people's access to health-related products and services in Iran. This research aimed to improve the negative state of the household's health. Over the last three decades, there has been a positive trend in raising society's level of health, reducing epidemics, and raising health indicators.
Based on the tables, certain variables have decreased at low levels of
The results show that the lower the
The results suggest that the lower the
Conclusion
A change in the consumption expenditure of other goods and the family's preferences will result from the implementation of any government policy or a shift in the household's attitude. This increases health expenmditures compared to the total consumption bundle. The key takeaway is that the choice of consumption between commodities and services related to health and other items influences the amount of money spent on health-related goods and services. Therefore, researchers suggest that officials in this field encourage households to use health services. This is done by enhancing health and treatment facilities, or more precisely, raising the standard of health development across the nation, and expanding the availability of health insurance services. Give specific income to households with more members or lower incomes to avoid burdening them with large health expenditures, which will cause them to utilize these goods and services less. Additionally, various health facilities, organizations, and laws requiring universal insurance coverage may make it easier for households to receive services.
This study examines the effects of policy change on health expenditures of household behavior using the DSGE model. The reduction of total health expenditure has led to an increase in the consumption expenditure of other goods. This increases the household consumption and the welfare of society. The results of this research and modeling indicate that since the family has little tendency to spend a larger share of its total consumption expenditure on health services, an increase in health expenditure causes the household to reduce the consumption of other goods and services. As a result, the total utility of goods and services will fall.
On the other hand, the lower the parameter of household health expenditure, the stronger the impact of the shock on the consumption variable and the utility of other goods and services in the model. If the value of this parameter increases, the impact of the shock on the consumption variable and the utility of health goods and services will be stronger, and the impact of this shock will be more severe. The combination and selection of a household's consumption bundle of goods and services can change the results of shocks and behavior of households. Moreover, the health of households and society casts a shadow on their other activities. Any change in health costs should be considered, and government policies should be adjusted in order to improve health services.
Policies regarding the choice of consumption bundle of health services should be modified. This is because it has an impact on the health of family members and overshadows their other activities. Therefore, it is recommended that insurance coverage be expanded, insurance funds and government support for per capita insurance fees be combined, and household purchasing patterns be changed. This increases and facilitates household access to these services. On the other hand, hasty measures that support widespread health privatizations should be avoided.
Considering the existence of urban and rural households in the country, and the difference in household behavior caused by the government's policy, the author suggests that in the future researchers consider the separation of urban and rural households in their modeling and propose executive policies based on that.
Acknowledgments
The outhors would like to thank the anonymous reviewers and editors for their valuable contribution.
Conflict of interests
The author declared no conflict of interests.
Authors' contributions
Izadi HR designed research, conducted research, analyzed data, and wrote the paper. Izadi HR had primary responsibility for the final content. All authors read and approved the final manuscript.
Funding
Non applicable.
Type of Study: Original article |
Subject:
Health Economics
Received: 2022/07/20 | Accepted: 2022/10/26 | Published: 2022/12/31
Received: 2022/07/20 | Accepted: 2022/10/26 | Published: 2022/12/31
References
1. Aziz A, Permana I, Alfarisi M. Factors affecting household consumption pattern. Electronic Journal. 2018; 10: 140-56.
2. Rous JJ, Hotchkiss DR. Estimation of the determinants of household health care expenditures in Nepal with controls for endogenous illness and provider choice. Health Economics. 2003; 12(6): 431-51. [DOI: 10.1002/hec.727]
3. Zare H, Trujillo AJ, Leidman E, Buttorff Ch. Income elasticity of health expenditures in Iran. Health Policy Plan. 2013; 28(6): 665-79. [DOI: 10.1093/heapol/czs106]
4. Sanwald A, Theurl E. Out-of-pocket payments in the Austrian healthcare system - a distributional analysis. Int J Equity Health. 2015; 14: 94. [DOI: 10.1186/s12939-015-0230-7]
5. Osuji O. Effect of inflation on household final consumption expenditure in Nigeria. Journal of Economics and Development Studies. 2020; 8(1)10: 104-111. [DOI: 10.15640/jeds.v8n1a8]
6. Zeynalova Z, Mammadli M. Analysis of the economic factors affecting household consumption expenditures in Azerbaijan. Journal of Critical Reviews. 2020; 7(7): 241-8. [DOI: 10.31838/jcr.07.07.40]
7. Long JB, Plosser Charles I. Real business cycles. Journal of Political Economy. 1983; 91(1): 39–69.
8. Locky Liu X, Pagan AR, Robinson T. Critically assessing estimated DSGE models: A case study of a multi-sector model. Economic Record. 2018; 94(5): 349-71. [DOI: 10.1111/1475-4932.12425]
9. Clarida R, Jordi G, Mark G. The science of monetary policy: a new Keynesian perspective. Journal of Economic Literature. 1999; 37(4): 1661–707. [DOI: 10.1257/jel.37.4.1661]
10. Gali J. Monetary policy, inflation and the business cycle: An introduction to the new Keynesian framework and its applications. New Jersy: Princeton University Press; 2007.
11. Grossman M. On the concept of health capital and the demand for health. Journal of Political Economy.1972; 80(2): 223-55.
12. Gerdham U, Lothgren M. New panel results on cointegration of international health expenditure and GDP. Applied Economics. 2000; 34(13): 1679-86. [DOI: 10.1080/00036840110116397.]
13. Getzen ThE. Healthcare is an individual necessity and a national luxury: Applying multilevel decision models to the analysis of health care expenditures. Journal of Health Economics. 2000; 19(2): 259-70. [DOI: 10.1016/s0167-6296(99)00032-6]
14. Guisan MC, Arranz M. Econometric models of private and public health expenditure in oecd countries, 1970-96. Applied Econometrics and International Development. 2003; 3(3): 49-60.
15. Matsaganis M, Mitrakos Th, Tsakloglou P. Modelling health expenditure at the household level in greece. The European Journal of Health Economics. 2009; 10(3): 329-36. [DOI: 10.1007/s10198-008-0137-y]
16. Mullahy J. Econometric modeling of health care costs and expenditures: A survey of analytical issues and related policy considerations. Medical Care. 2009; 47(7): 104-8. [DOI: 10.1097/MLR.0b013e31819c9593]
17. Wang KM. Health care expenditure and economic growth: Quantile panel-type analysis. Economic Modelling. 2011; 28(4): 1536–49. [DOI: 10.1016/j.econmod.2011.02.008]
18. Malik AM, Azam Syed ShI. Socio-economic determinants of household out-of-pocket payments on healthcare in Pakistan. International Journal for Equity in Health. 2012; 11: 51. [DOI: 10.1186/1475-9276-11-51]
19. Lee W, Jiang L, Phillips ChD, Ohsfeldt RL. Rural-urban differences in health care expenditures: Empirical data from us households. Advances in Public Health. 2014; 43: 57-80. [DOI: 10.1155/2014/435780]
20. Brown S, Hole AR, Kilic D. Out-of-pocket health care expenditure in turkey: Analysis of the 2003–2008 household budget surveys. Economic Modelling. 2014; 41: 211-8. [DOI: 10.1016/j. econmod.2014.05.012]
21. Smets F, Wouters R. An estimated dynamic stochastic general equilibrium model of the euro area. Journal of the European Economic Association. 2003; 1(5): 1123-75. [DOI: 10.1162/ 154247603770383415]
22. Izadi HR. Investigation of the role of change in utility function components and its effect on smooth the dynamic movement path of model variables. Studies In Business and Economics. 2022; 17(1): 73-84. [DOI: 10.2478/sbe-2022-0005]
23. Izadi HR, Marzban H. The role of productivity growth changes in determining optimal monetary and fiscal policies from the Ramsey problem. Quarterly Journal of Quantitative Economics. 2016; 16(2): 37-71. [In Persian]
24. Izadi HR. The role of tendency of government preference in an optimal fiscal policy model in the presence of agent heterogeneity in a DSGE framework. Quarterly Journal of Economical Modelling. 2019; 12(44): 73-96. [In Persian]
25. Izadi HR. Investigating the role of financial sanctions in utility function and their impact on household behavior. DLSU Business & Economics Review. 2021; 31(1): 132-141.
26. Izadi HR, Sayareh, M. Investigating the role of labor division into internal and external sectors in the Iranian economy within the framework of dynamic stochastic general equilibrium model. Journal of Econometric Modelling. 2019; 4(3): 87-110. [In Persian] [DOI: 10.22075/jem.2019.18181.1339]
27. Izadi HR, Marzban H. Designing, investigation and comparison of the factors of stationarity of dynamic stochastic general equilibrium models in Iran economy. Quarterly Journal of Economic Research and Policies. 2017; 24(80): 195–216. [In Persian]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
