

Volume 9, Issue 3 (10-2025)
EBHPME 2025, 9(3): 198-205 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Saghaeiannejad-Isfahani S, Esmailzadeh M, Pouriaye Vali B, Rezaei A. A Narrative Review of Health Observatory: Framework, Challenges, and Future Prospects in National and Global Systems. EBHPME 2025; 9 (3) :198-205
URL: http://jebhpme.ssu.ac.ir/article-1-546-en.html
URL: http://jebhpme.ssu.ac.ir/article-1-546-en.html



Health Information Technology Research Center, Department of Health Information Technology Management, Faculty of Medical Management and Informatics, Isfahan University of Medical Sciences, Isfahan, Iran , Abolfazlrezaei2013@yahoo.com
Keywords: Health Observatory, Health Surveillance, National Health Observatory (NHO), Global Health Observatory
Full-Text [PDF 1176 kb]
(110 Downloads)
| Abstract (HTML) (647 Views)
Introduction
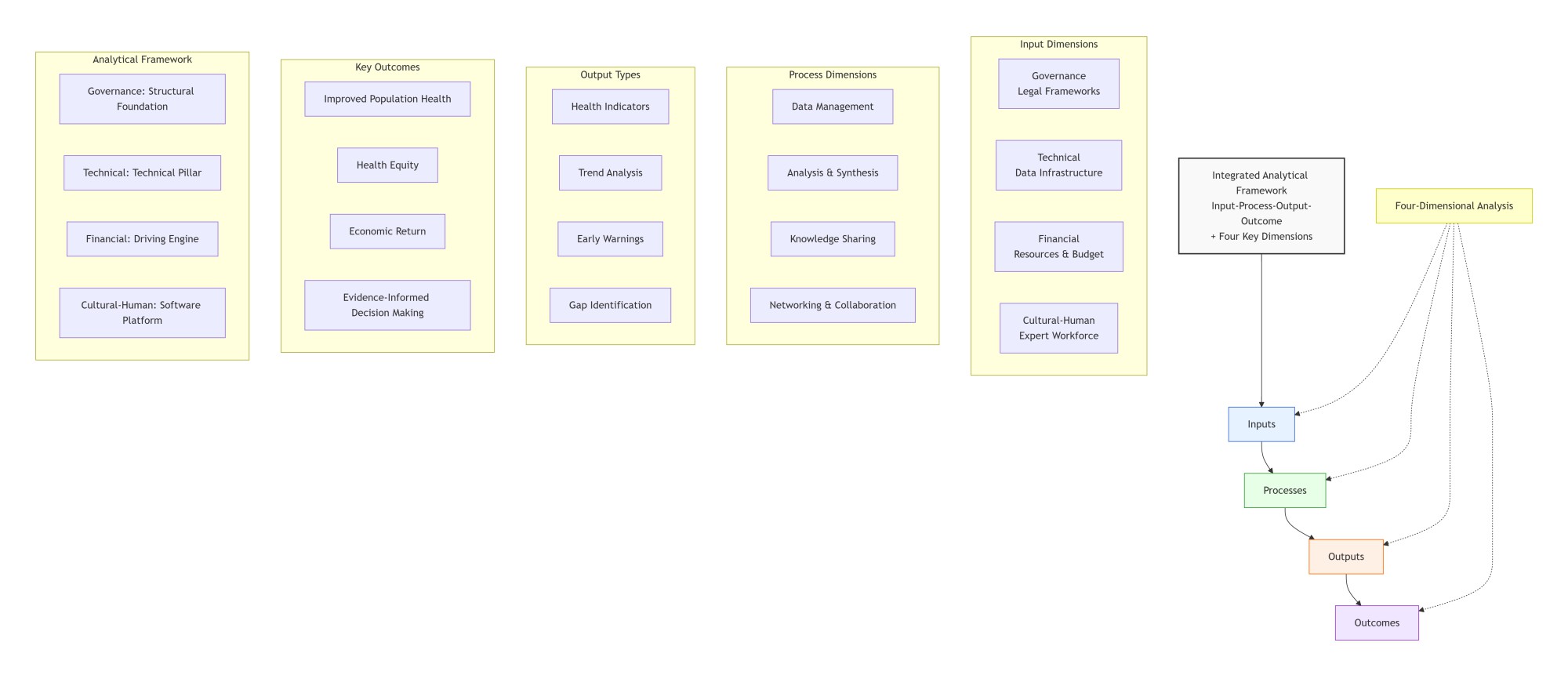
Figure 1. Integrated Analytical Framework for Health Observatory Systems: Linking Inputs, Processes, Outputs, and Outcomes across Four Key Dimensions
Full-Text: (56 Views)
| A B S T R A C T Introduction: In an era marked by global health crises and data-driven policymaking, timely and accurate health data are indispensable for assessing population health and achieving Sustainable Development Goals (SDGs) and Universal Health Coverage (UHC). Health observatories serve as integrated platforms for collecting, analyzing, and disseminating health data, thereby enhancing evidence-informed decision-making and strengthening health systems. Materials and Methods: This structured narrative review was chosen to accommodate the complexity and multidimensionality of health observatory systems. The PRISMA-ScR framework guided the review process, ensuring methodological rigor, transparency, and reproducibility. Results: Findings were synthesized using an input–process–output–outcome framework across four dimensions: governance, technical, financial, and cultural–human. This model facilitated a comprehensive analysis of the structures, capacities, and challenges of health observatories, drawing on examples from national and global initiatives. Conclusion: To ensure sustainability and effectiveness, countries must invest in robust governance, advanced data infrastructure, skilled human resources, and a culture of data-driven decision-making. Strengthening these pillars will accelerate progress toward UHC and SDGs, and foster resilient health systems worldwide. Keywords: Health Observatory, Health Surveillance, National Health Observatory (NHO), Global Health Observatory |
Introduction
In an era of increasing global health challenges and data-driven policymaking, timely and accurate health data are essential for assessing population health, setting priorities, and monitoring progress toward key objectives such as the Sustainable Development Goals (SDGs) and Universal Health Coverage (UHC) (1, 2).
The concept of a “Health Observatory” emerged in the mid-1970s as a comprehensive and integrated platform for generating high-quality, reliable information on human health and healthcare systems. Since then, numerous national and regional observatories have been established worldwide, reflecting growing recognition of their role in strengthening health governance (3).
The structure and functionality of health observatories vary across countries and regions, influenced by their level of development and institutional capacity (4). Many nations have adopted observatories to address fragmentation in their health information systems. Regional initiatives and the World Health Organization’s Global Health Observatory further illustrate the expanding scope of these platforms (5).
National Health Observatories (NHOs) aim to improve access to and use of health data related to status, trends, and social determinants. They support political dialogue, strategic planning, and evaluation of national health goals. Core functions include data collection, surveillance, analysis, and dissemination, with the overarching goal of enabling evidence-based decision-making and enhancing service delivery across health systems (6).
For example, countries in the African region, with support from WHO, have implemented NHOs to strengthen their National Health Information Systems (NHIS). These efforts have focused on clarifying priorities, identifying challenges, and formulating strategies to improve observatory performance (6).
Despite progress, several challenges persist: conceptual ambiguity surrounding “observatories,” unclear legal frameworks, overlapping institutional roles, limited skilled workforce, and inadequate ICT infrastructure (1, 6).
Today, a diverse array of observatories operate globally, including the WHO Global Observatory on Health Research and Development (7), the WHO Global eHealth Observatory (8), the International Observatory on Mental Health Systems (9), and the National Public Health Observatory of Cameroon (1). In Iran, recent efforts have proposed a Women’s Health Research Surveillance System based on a networked model linking research and executive centers (10).
Although global interest in health observatories is growing, many countries still face structural, legal, and technological barriers to their effective implementation. Strengthening these systems is essential for achieving SDGs and UHC, particularly in countries like Iran that are developing specialized health surveillance platforms.
This study aims to provide a comprehensive review of the frameworks, applications, challenges, and strategic approaches to developing health observatories at national and global levels. By synthesizing theoretical and practical insights, the study seeks to support evidence-informed policymaking and enhance health system performance.
Materials and Methods
Study Design
This study was conducted as a structured narrative review to analyze the frameworks, practical experiences, challenges, and opportunities related to health observatories and surveillance systems at national, regional, and global levels.
Data sources and search strategy
A comprehensive literature search was performed using major scientific databases, including PubMed, Scopus, Web of Science, and Google Scholar. Additionally, gray literature from authoritative sources—such as the World Health Organization (WHO), the Global Health Observatory, the World Bank, and other specialized institutions—was reviewed.
The primary search terms included: “health observatory,” “national health observatory,” “global health observatory,” and “health observatory system,” along with their Persian equivalents. Boolean operators (AND, OR) were also used to refine the search.
For example, the PubMed search strategy was: (("health observatory"[Title/Abstract] OR "national health observatory"[Title/Abstract] OR "global health observatory"[Title/Abstract]) AND ("framework"[Title/Abstract] OR "model"[Title/Abstract] OR "structure"[Title/Abstract] OR "challenge*"[Title/Abstract] OR "experience "[Title/Abstract] OR "implementation"[Title/Abstract]))
The search focused on literature published between 2010 and 2025, although foundational sources from earlier years were also included when relevant.
Inclusion and Exclusion Criteria
Inclusion criteria
The concept of a “Health Observatory” emerged in the mid-1970s as a comprehensive and integrated platform for generating high-quality, reliable information on human health and healthcare systems. Since then, numerous national and regional observatories have been established worldwide, reflecting growing recognition of their role in strengthening health governance (3).
The structure and functionality of health observatories vary across countries and regions, influenced by their level of development and institutional capacity (4). Many nations have adopted observatories to address fragmentation in their health information systems. Regional initiatives and the World Health Organization’s Global Health Observatory further illustrate the expanding scope of these platforms (5).
National Health Observatories (NHOs) aim to improve access to and use of health data related to status, trends, and social determinants. They support political dialogue, strategic planning, and evaluation of national health goals. Core functions include data collection, surveillance, analysis, and dissemination, with the overarching goal of enabling evidence-based decision-making and enhancing service delivery across health systems (6).
For example, countries in the African region, with support from WHO, have implemented NHOs to strengthen their National Health Information Systems (NHIS). These efforts have focused on clarifying priorities, identifying challenges, and formulating strategies to improve observatory performance (6).
Despite progress, several challenges persist: conceptual ambiguity surrounding “observatories,” unclear legal frameworks, overlapping institutional roles, limited skilled workforce, and inadequate ICT infrastructure (1, 6).
Today, a diverse array of observatories operate globally, including the WHO Global Observatory on Health Research and Development (7), the WHO Global eHealth Observatory (8), the International Observatory on Mental Health Systems (9), and the National Public Health Observatory of Cameroon (1). In Iran, recent efforts have proposed a Women’s Health Research Surveillance System based on a networked model linking research and executive centers (10).
Although global interest in health observatories is growing, many countries still face structural, legal, and technological barriers to their effective implementation. Strengthening these systems is essential for achieving SDGs and UHC, particularly in countries like Iran that are developing specialized health surveillance platforms.
This study aims to provide a comprehensive review of the frameworks, applications, challenges, and strategic approaches to developing health observatories at national and global levels. By synthesizing theoretical and practical insights, the study seeks to support evidence-informed policymaking and enhance health system performance.
Materials and Methods
Study Design
This study was conducted as a structured narrative review to analyze the frameworks, practical experiences, challenges, and opportunities related to health observatories and surveillance systems at national, regional, and global levels.
Data sources and search strategy
A comprehensive literature search was performed using major scientific databases, including PubMed, Scopus, Web of Science, and Google Scholar. Additionally, gray literature from authoritative sources—such as the World Health Organization (WHO), the Global Health Observatory, the World Bank, and other specialized institutions—was reviewed.
The primary search terms included: “health observatory,” “national health observatory,” “global health observatory,” and “health observatory system,” along with their Persian equivalents. Boolean operators (AND, OR) were also used to refine the search.
For example, the PubMed search strategy was: (("health observatory"[Title/Abstract] OR "national health observatory"[Title/Abstract] OR "global health observatory"[Title/Abstract]) AND ("framework"[Title/Abstract] OR "model"[Title/Abstract] OR "structure"[Title/Abstract] OR "challenge*"[Title/Abstract] OR "experience "[Title/Abstract] OR "implementation"[Title/Abstract]))
The search focused on literature published between 2010 and 2025, although foundational sources from earlier years were also included when relevant.
Inclusion and Exclusion Criteria
Inclusion criteria
- Study types: Primary research (quantitative, qualitative, or mixed methods), review articles (systematic or narrative), technical reports, policy documents, and official publications
- Languages: English and Persian
- Content: Sources addressing definitions, structures, functions, challenges, opportunities, or successful examples of health observatories
Exclusion criteria
- Promotional or news-based content
- Sources lacking conceptual analysis or empirical evidence
Screening and Data Extraction
All references were managed using Mendeley software. After removing duplicates, titles and abstracts were screened independently by two researchers based on the inclusion and exclusion criteria. Full texts of eligible sources were then reviewed, and key data were extracted.
Extracted data included
All references were managed using Mendeley software. After removing duplicates, titles and abstracts were screened independently by two researchers based on the inclusion and exclusion criteria. Full texts of eligible sources were then reviewed, and key data were extracted.
Extracted data included
- Title and source
- Type of study or document
- Geographical level (national, regional, global)
- Definitions and theoretical frameworks
- Structural or implementation models
- Evaluation indicators and performance metrics
- Challenges, barriers, opportunities, and reported outcomes
Inter-rater agreement during the initial screening was assessed using Cohen’s Kappa coefficient, yielding a value of 0.82, and indicating excellent agreement. In cases of disagreement—especially regarding gray literature or ambiguous sources—a third reviewer (a faculty expert in health information systems) was consulted to reach consensus.
Data Analysis
Data were analysed using qualitative and descriptive methods. Findings were organized within a predefined thematic framework encompassing:
Data Analysis
Data were analysed using qualitative and descriptive methods. Findings were organized within a predefined thematic framework encompassing:
- Theoretical foundations (definitions, principles, conceptual models)
- Practical applications (national and global examples)
- Challenges and proposed solutions
- Future opportunities and foresight analysis
This structured approach enabled a coherent synthesis of findings and supported the development of evidence-based policy recommendations.
Results
Conceptual Framework
The findings were synthesized using an input–process–output–outcome model, structured around four key dimensions: governance, technical, financial, and cultural–human determinants. This framework enabled a comprehensive and coherent analysis of health observatory systems, addressing their components, capacities, challenges, and impacts.
Inputs: Infrastructure, Resources, and Capacities
Effective health observatories require robust data infrastructure, standardized protocols, advanced technologies (11, 20), skilled human resources, and legally grounded governance. However, financial disparities—especially in low-income countries contributing only 1% to global R&D—create significant gaps in data collection and analysis (24). Sustainable financing models, such as public–private partnerships and cost-effectiveness analysis, are essential for long-term viability (31). Culturally, fostering a data-driven mind-set and investing in workforce development are critical success factors (12, 20).
Processes: Data Management, Analysis, and Governance
Core processes include continuous data collection, transformation of raw data into actionable insights, transparent dissemination, and intersect oral collaboration (6, 14, 15). Managerial challenges—like coordination and cultural resistance—can be addressed through:
Results
Conceptual Framework
The findings were synthesized using an input–process–output–outcome model, structured around four key dimensions: governance, technical, financial, and cultural–human determinants. This framework enabled a comprehensive and coherent analysis of health observatory systems, addressing their components, capacities, challenges, and impacts.
Inputs: Infrastructure, Resources, and Capacities
Effective health observatories require robust data infrastructure, standardized protocols, advanced technologies (11, 20), skilled human resources, and legally grounded governance. However, financial disparities—especially in low-income countries contributing only 1% to global R&D—create significant gaps in data collection and analysis (24). Sustainable financing models, such as public–private partnerships and cost-effectiveness analysis, are essential for long-term viability (31). Culturally, fostering a data-driven mind-set and investing in workforce development are critical success factors (12, 20).
Processes: Data Management, Analysis, and Governance
Core processes include continuous data collection, transformation of raw data into actionable insights, transparent dissemination, and intersect oral collaboration (6, 14, 15). Managerial challenges—like coordination and cultural resistance—can be addressed through:
- Transformational leadership to promote evidence use
- Participatory management to engage stakeholders
- Capacity building through specialized training, along with strong governance, national ownership, and harmonized policies, ensures process sustainability (1, 6, 20).
Outputs: Actionable Data and Information
Outputs include health indicators, trend analyses, data gap identification, and early warning alerts. Standardized, high-quality, and publicly accessible data empower policymakers and the public to make informed decisions. These outputs also support equity analysis, workforce planning, and pandemic preparedness (9, 13, 17, 19, 21, 27, 29, 30).
Outcomes: Health Equity and Economic Returns
Health observatories reduce disparities and improve health outcomes by enabling data-driven policies and enhancing transparency (27, 28). Economically, they offer high returns through cost savings, efficiency gains, and improved prevention strategies (24, 31). Sustainable development depends on reinforcing governance, technology, financing, and culture (6, 12, 31).
Four-Dimensional Analysis: Challenges and Strategic Responses
Outputs include health indicators, trend analyses, data gap identification, and early warning alerts. Standardized, high-quality, and publicly accessible data empower policymakers and the public to make informed decisions. These outputs also support equity analysis, workforce planning, and pandemic preparedness (9, 13, 17, 19, 21, 27, 29, 30).
Outcomes: Health Equity and Economic Returns
Health observatories reduce disparities and improve health outcomes by enabling data-driven policies and enhancing transparency (27, 28). Economically, they offer high returns through cost savings, efficiency gains, and improved prevention strategies (24, 31). Sustainable development depends on reinforcing governance, technology, financing, and culture (6, 12, 31).
Four-Dimensional Analysis: Challenges and Strategic Responses
- Governance: Requires clear legal frameworks and intersectoral coordination (1, 6, 20).
- Technical: Depends on infrastructure and analytical expertise (6, 14, 15).
- Financial: Is threatened by lack of sustainable models and investment inequities (24).
- Cultural–Human: Faces workforce shortages and resistance to data sharing
- Managerial challenges: can be mitigated through phased planning and structured change management (6, 12).
Pathway to Sustainable Development
Integrated strategies across all four dimensions are essential for successful observatory systems. Strengthening these areas enables effective data use, rapid response to health threats, and sustained evidence-based policymaking (6, 12, 31).
Synthesis and Analytical Framework
This synthesis of findings provides a structured, precise, and coherent framework for analysing and improving health observatory systems, offering both comprehensiveness and analytical rigor to meet research and practical needs in the field. The study’s findings were reorganized using an input–process–output–outcome conceptual model, with a focus on four key dimensions: governance, technical, financial, and cultural–human determinants. This analytical framework enables simultaneous examination of system components, types, capacities, challenges, and impacts, while directly addressing reviewers’ critiques regarding the need for a clear theoretical foundation and the inclusion of economic and managerial analysis. The overall structure and interrelation of these dimensions are visually summarized in Figure 1, which illustrates the conceptual pathway toward sustainable and effective health observatory systems.
Integrated strategies across all four dimensions are essential for successful observatory systems. Strengthening these areas enables effective data use, rapid response to health threats, and sustained evidence-based policymaking (6, 12, 31).
Synthesis and Analytical Framework
This synthesis of findings provides a structured, precise, and coherent framework for analysing and improving health observatory systems, offering both comprehensiveness and analytical rigor to meet research and practical needs in the field. The study’s findings were reorganized using an input–process–output–outcome conceptual model, with a focus on four key dimensions: governance, technical, financial, and cultural–human determinants. This analytical framework enables simultaneous examination of system components, types, capacities, challenges, and impacts, while directly addressing reviewers’ critiques regarding the need for a clear theoretical foundation and the inclusion of economic and managerial analysis. The overall structure and interrelation of these dimensions are visually summarized in Figure 1, which illustrates the conceptual pathway toward sustainable and effective health observatory systems.
Figure 1. Integrated Analytical Framework for Health Observatory Systems: Linking Inputs, Processes, Outputs, and Outcomes across Four Key Dimensions
Discussion
This review aimed to comprehensively analyze the frameworks, applications, and challenges of
health observatory systems at national and international levels. The findings highlight that health observatories are not merely data repositories but strategic platforms essential for assessing population health, monitoring progress, and enabling evidence-informed policymaking (1, 13). Their emergence since the 1970s and growing global adoption reflect the urgent need for integrated health information systems (4, 6).
Alignment with Literature
The role of health observatories in reducing health inequities and supporting data-driven decisions aligns with existing research (5, 16, 28). Studies by Kebede, Zielinski, and Ndongue emphasize their importance in addressing data scarcity and strengthening health information systems, particularly in low-resource settings (3, 5, 6).
Functional Dimensions
Health observatories operate across four core functions: data marshalling, analysis and synthesis, information dissemination, and stakeholder networking (6, 15). These functions enable the transformation of raw data into actionable insights, support early warning systems, and foster collaboration across sectors to promote health equity (16, 28).
Diversity and Localization
Global evidence reveals a wide variety of observatory models—from the WHO’s Global Health Observatory (GHO) to specialized platforms like GoPA and national systems in Iran and Cameroon (2, 4, 13, 20, 27). This diversity underscores the need for flexible, context-specific designs tailored to national priorities and capacities.
Challenges and Strategic Solutions
Despite progress, observatories face multidimensional challenges across governance, technical, financial, and cultural domains (8, 25, 30):
This review aimed to comprehensively analyze the frameworks, applications, and challenges of
health observatory systems at national and international levels. The findings highlight that health observatories are not merely data repositories but strategic platforms essential for assessing population health, monitoring progress, and enabling evidence-informed policymaking (1, 13). Their emergence since the 1970s and growing global adoption reflect the urgent need for integrated health information systems (4, 6).
Alignment with Literature
The role of health observatories in reducing health inequities and supporting data-driven decisions aligns with existing research (5, 16, 28). Studies by Kebede, Zielinski, and Ndongue emphasize their importance in addressing data scarcity and strengthening health information systems, particularly in low-resource settings (3, 5, 6).
Functional Dimensions
Health observatories operate across four core functions: data marshalling, analysis and synthesis, information dissemination, and stakeholder networking (6, 15). These functions enable the transformation of raw data into actionable insights, support early warning systems, and foster collaboration across sectors to promote health equity (16, 28).
Diversity and Localization
Global evidence reveals a wide variety of observatory models—from the WHO’s Global Health Observatory (GHO) to specialized platforms like GoPA and national systems in Iran and Cameroon (2, 4, 13, 20, 27). This diversity underscores the need for flexible, context-specific designs tailored to national priorities and capacities.
Challenges and Strategic Solutions
Despite progress, observatories face multidimensional challenges across governance, technical, financial, and cultural domains (8, 25, 30):
- Governance: Conceptual ambiguity, weak coordination, and lack of legal clarity hinder efficiency (1, 6, 12, 31).
- Technical: Data inconsistency, poor infrastructure, and low quality limit effectiveness (2, 4, 12, 20, 27).
- Financial: Limited investment and unsustainable models threaten continuity (12, 20, 25).
- Cultural–Human: Resistance to data sharing and workforce shortages persist (1, 6, 12, 26).
Addressing these challenges requires integrated, phased reforms that align legal, technical, financial, and cultural strategies. These dimensions and their interrelations are illustrated in Figure 1, which presents a conceptual pathway for sustainable observatory development.
Future Directions
Strategic advancement of health observatories should begin with governance reform, followed by investment in infrastructure, human capacity development, and cultural transformation (12, 31). Establishing localized observatory networks—such as Iran’s Women’s Health Research Observatory—can ensure relevance, sustainability, and impact. These systems must evolve as dynamic, context-sensitive platforms capable of responding to emerging health challenges and supporting long-term policy goals.
Conclusion
This review provided a comprehensive analysis of the roles, functions, types, and challenges of health observatory systems at global, national, and local levels. Health observatories are strategic and essential platforms for assessing health status, monitoring progress, and supporting evidence-informed policymaking (1, 4, 13). Their core functions—data marshaling, analysis and synthesis, information sharing, and stakeholder networking—collectively transform raw data into actionable knowledge, improve health outcomes, and enable informed decision-making (4, 15, 16).
Despite their strategic importance, health observatories face multidimensional challenges across governance, technological infrastructure, human and financial resources, and cultural domains. These barriers undermine their sustainability and effectiveness (3, 12, 23). Overcoming them requires a coordinated approach that includes strengthening governance mechanisms, investing in data and technology, developing specialized human capacity, and fostering a data-driven culture (3, 12, 23).
This study contributes to the existing literature by offering a structured framework and in-depth analysis of health observatory systems, with particular attention to underexplored dimensions in low- and middle-income countries. The findings can inform future research aimed at evaluating interventions and developing localized observatory models.
Importantly, health observatories must evolve beyond passive data repositories. They should actively engage in the decision-making process by producing concise, analytical reports and facilitating policy dialogue. Achieving this requires a deep understanding of system dynamics and a strong culture of data analysis within each country. Such an approach—illustrated in the conceptual framework (Figure 1)—will enhance transparency, accountability, and the continuous improvement of service quality and equity in health systems.
Ethical considerations
In this review, we attempted to evaluate the literature based on scientific criteria and not on non -scientific factors such as gender, race, ethnicity, religion, or socioeconomic status.
Acknowledgments
The authors would like to express their sincere gratitude to all individuals who contributed to the completion of this study. Special thanks are extended to Dr. Sakineh Saghaeiannejad-Isfahani for her valuable guidance and expertise throughout the research process.
Conflict of interests
The authors declared no conflict of interests.
Authors’ contributions
All authors actively contributed to the writing and development of this article. M.E and B.P jointly conducted the systematic searches across databases and performed the initial screening of articles. In addition to her role in the search process, M.S was responsible for drafting the introduction and methodology sections. B.P carried out the data analysis and authored the findings section. A.R led the writing of the discussion and final conclusion sections and provided scientific oversight throughout all stages of the research. Additionally, S.S. contributed to the critical review of the manuscript, participated in data interpretation, and finalized the submitted version. All authors read and approved the final manuscript and take full responsibility for the accuracy and integrity of its content.
Funding
No funding was received for this study.
References
1. Ndoungue VF, Tiwoda C, Gnigninanjouena O, Bataliack S, Mbondji E, Labat A. National Health Observatory: A tool to strengthen the health information system for evidence-based decision making and health policy formulation in Cameroon. Health Policy OPEN. 2022;3:100085. DOI:10.1016/j.hpopen.2022.100085
2. Vardell E. Global Health Observatory Data Repository. Med Ref Serv Q (Internet). 2020;39(1):67–74. DOI:10.1080/02763869. 2019. 1693231
3. Kebede D, Zielinski C, Mbondji PE, Piexoto M, Kouvividila W, Sambo LG. The african health observatory and national health observatories as platforms for strengthening health information systems in sub-saharan africa. J R Soc Med. 2014;107:6–9.
4. Rashidian A, Damari B, Larijani B, Vosoogh Moghaddam A, Alikhani S, Shadpour K, et al. Health observatories in Iran. Iran J Public Health. 2013;42(1 SUPPL 1):84–7.
5. Kebede D, Zielinski C. The potential role of regional and national health observatories in narrowing the knowledge gap in sub-Saharan Africa. J R Soc Med. 2014;107:3–5.
6. Serge B, Ebongue M, Saha Tahoum UA, Tania BL, Humphrey K. Focus, priorities, and challenges of National Health Observatories (NHOs) in Africa. Available at SSRN 4661902. 2023.
7. Adam T, Røttingen JA, Kieny MP. Informing the establishment of the who global observatory on health research and development: A call for papers. Heal Res Policy Syst. 2015;13(1):3–6.
8. Ryu S. Book Review: mHealth: New horizons for health through mobile technologies: based on the findings of the second global survey on ehealth (global observatory for ehealth series, volume 3). Health Inform Res. 2012;18(3):231.
9. Minas H. International observatory on mental health systems: Structure and operation. Int J Ment Health Syst. 2009;3:1–9.
10. Rostami Goran N, Ahmadi B, Baghian N, Farzadi F. Women’s health research observeier system: A model for research networking. Iran J Cult Health Promot 2024; 7 (4) :513-521.
11. Guidotti TL. The observatory: A model for studies in health, society, and the environment. J Environ Stud Sci (Internet). 2022;12(4):827–37.
DOI:10.1007/s13412-022-00786-6
12.Pooransingh S, Misir A, Ramdath D, Ramsewak S, Jaglal S, Cameron C, et al. Barriers and facilitators to establishing a national public health observatory. Rev Panam Salud Publica/Pan Am J Public Heal. 2015;38(5):403–9.
13. Damari B, Heidari A, Rashidian A, Vosoogh Moghaddam A, Khosravi A, Alikhani S. Designing a health observatory system for the Islamic Republic of Iran. Payesh 2020; 19 (5) :499-509.
14. Pourmalek F. National health observatories: Need for stepped-up action. The Health. 2012;3(3):63–4.
15. Barcellos C, Roux E, Ceccato P, Gosselin P, Monteiro AM, De Matos VP, et al. An observatory to gather and disseminate information on the health-related effects of environmental and climate change. Rev Panam Salud Publica/Pan Am J Public Heal. 2016;40(3):167–73.
16. Madela-Mntla EN, Jeenah M, Loots G, Mayosi BM. The development of a national health research observatory in south africa: Considerations and challenges. South African Heal Rev. 2016;2016(1): 235–41.
17. Varela AR, Hallal PC, Grueso JM, Pedišić Ž, Salvo D, Nguyen A, et al. Status and trends of physical activity surveillance, policy, and research in 164 countries: findings from the global observatory for physical activity—gopa! 2015 and 2020 surveys. J Phys Act Heal. 2023;20(2):112–28.
18. Milton K, Cavill N, Chalkley A, Foster C, Gomersall S, Hagstromer M, et al. Eight investments that work for physical activity. J Phys Act Heal. 2021;18(6):625–30.
19. Mina MJ, Metcalf CJE, McDermott AB, Douek DC, Farrar J, Grenfell BT. A global lmmunological observatory to meet a time of pandemics. Elife. 2020;9:1–5.
20. Mehrolhassani M, Amiresmaili M, Iranmanesh M. An evaluation model for monitoring human resources in the health system of iran . Irje. 2019;14 :40-9.
21. Farzadi F, Montazeri A, Sadighi J, Aeenparast A, Tavousi M, Maftoon F, et al. Observation of the implementation of the article 11 of general health policies in iran: the study protocol. Iran J Cult Health Promot. 2019;2(3):326-32.
22. Dias MA de S, Friche AA de L, Oliveira VB de, Caiaffa WT. The belo horizonte observatory for urban health: its history and current challenges. Cad Saude Publica. 2015;31(suppl 1):277–85.
23. Gigantesco A, Giuliani M, Graziano S, Zaami S, Tittarelli R, Pichini S, et al. The complex and constantly evolving public health threat of new psy. Ann Ist Super Sanità. 2011;47(4):363–72.
24. Røttingen JA, Regmi S, Eide M, Young AJ, Viergever RF, Ardal C, et al. Mapping of available health research and development data: what’s there, what’s missing, and what role is there for a global observatory? Lancet (Internet). 2013;382(9900):1286–307.
DOI:10.1016/S0140-6736(13)61046-6
25.Varela AR, Pratt M, Powell K, Lee IM, Bauman A, Heath G, et al. Worldwide surveillance, policy, and research on physical activity and health: The global observatory for physical activity. J Phys Act Heal. 2017;14(9):701–9.
26.Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global health workforce labor market projections for 2030. Hum Resour Health. 2017;15(1):1–12.
27. Zaveri A, Lehmann J, Auer S, Hassan MM, Sherif MA, Martin M. Publishing and interlinking the global health observatory dataset. Semant Web. 2013;4(3): 315–22.
28. Ramirez Varela A, Salvo D, Pratt M, Milton K, Siefken K, Bauman A, et al. Worldwide use of the first set of physical activity Country Cards: The Global Observatory for Physical Activity - GoPA! Int J Behav Nutr Phys Act. 2018;15(1):1–14.
29. Onagbiye S, Ricci H, Bester P, Ricci C. Sedentariness and overweight in relation to mortality in sub-Saharan Africa. A mediation analysis based on the World Health Organization-Global Health Observatory data repository. J Public Health Africa. 2023;14(4):71–6.
30. Li C, He WQ. Comparison of primary liver cancer mortality estimates from World Health Organization, global burden disease and global cancer observatory. Liver Int. 2022;42(10):2299–316.
31. Healy JM, Tang S, Patcharanarumol W, Annear PL.
A framework for comparative analysis of health systems: experiences from the Asia Pacific observatory on health systems and policies. WHO South-East Asia J public Heal. 2018;7(1):5–12.
Future Directions
Strategic advancement of health observatories should begin with governance reform, followed by investment in infrastructure, human capacity development, and cultural transformation (12, 31). Establishing localized observatory networks—such as Iran’s Women’s Health Research Observatory—can ensure relevance, sustainability, and impact. These systems must evolve as dynamic, context-sensitive platforms capable of responding to emerging health challenges and supporting long-term policy goals.
Conclusion
This review provided a comprehensive analysis of the roles, functions, types, and challenges of health observatory systems at global, national, and local levels. Health observatories are strategic and essential platforms for assessing health status, monitoring progress, and supporting evidence-informed policymaking (1, 4, 13). Their core functions—data marshaling, analysis and synthesis, information sharing, and stakeholder networking—collectively transform raw data into actionable knowledge, improve health outcomes, and enable informed decision-making (4, 15, 16).
Despite their strategic importance, health observatories face multidimensional challenges across governance, technological infrastructure, human and financial resources, and cultural domains. These barriers undermine their sustainability and effectiveness (3, 12, 23). Overcoming them requires a coordinated approach that includes strengthening governance mechanisms, investing in data and technology, developing specialized human capacity, and fostering a data-driven culture (3, 12, 23).
This study contributes to the existing literature by offering a structured framework and in-depth analysis of health observatory systems, with particular attention to underexplored dimensions in low- and middle-income countries. The findings can inform future research aimed at evaluating interventions and developing localized observatory models.
Importantly, health observatories must evolve beyond passive data repositories. They should actively engage in the decision-making process by producing concise, analytical reports and facilitating policy dialogue. Achieving this requires a deep understanding of system dynamics and a strong culture of data analysis within each country. Such an approach—illustrated in the conceptual framework (Figure 1)—will enhance transparency, accountability, and the continuous improvement of service quality and equity in health systems.
Ethical considerations
In this review, we attempted to evaluate the literature based on scientific criteria and not on non -scientific factors such as gender, race, ethnicity, religion, or socioeconomic status.
Acknowledgments
The authors would like to express their sincere gratitude to all individuals who contributed to the completion of this study. Special thanks are extended to Dr. Sakineh Saghaeiannejad-Isfahani for her valuable guidance and expertise throughout the research process.
Conflict of interests
The authors declared no conflict of interests.
Authors’ contributions
All authors actively contributed to the writing and development of this article. M.E and B.P jointly conducted the systematic searches across databases and performed the initial screening of articles. In addition to her role in the search process, M.S was responsible for drafting the introduction and methodology sections. B.P carried out the data analysis and authored the findings section. A.R led the writing of the discussion and final conclusion sections and provided scientific oversight throughout all stages of the research. Additionally, S.S. contributed to the critical review of the manuscript, participated in data interpretation, and finalized the submitted version. All authors read and approved the final manuscript and take full responsibility for the accuracy and integrity of its content.
Funding
No funding was received for this study.
References
1. Ndoungue VF, Tiwoda C, Gnigninanjouena O, Bataliack S, Mbondji E, Labat A. National Health Observatory: A tool to strengthen the health information system for evidence-based decision making and health policy formulation in Cameroon. Health Policy OPEN. 2022;3:100085. DOI:10.1016/j.hpopen.2022.100085
2. Vardell E. Global Health Observatory Data Repository. Med Ref Serv Q (Internet). 2020;39(1):67–74. DOI:10.1080/02763869. 2019. 1693231
3. Kebede D, Zielinski C, Mbondji PE, Piexoto M, Kouvividila W, Sambo LG. The african health observatory and national health observatories as platforms for strengthening health information systems in sub-saharan africa. J R Soc Med. 2014;107:6–9.
4. Rashidian A, Damari B, Larijani B, Vosoogh Moghaddam A, Alikhani S, Shadpour K, et al. Health observatories in Iran. Iran J Public Health. 2013;42(1 SUPPL 1):84–7.
5. Kebede D, Zielinski C. The potential role of regional and national health observatories in narrowing the knowledge gap in sub-Saharan Africa. J R Soc Med. 2014;107:3–5.
6. Serge B, Ebongue M, Saha Tahoum UA, Tania BL, Humphrey K. Focus, priorities, and challenges of National Health Observatories (NHOs) in Africa. Available at SSRN 4661902. 2023.
7. Adam T, Røttingen JA, Kieny MP. Informing the establishment of the who global observatory on health research and development: A call for papers. Heal Res Policy Syst. 2015;13(1):3–6.
8. Ryu S. Book Review: mHealth: New horizons for health through mobile technologies: based on the findings of the second global survey on ehealth (global observatory for ehealth series, volume 3). Health Inform Res. 2012;18(3):231.
9. Minas H. International observatory on mental health systems: Structure and operation. Int J Ment Health Syst. 2009;3:1–9.
10. Rostami Goran N, Ahmadi B, Baghian N, Farzadi F. Women’s health research observeier system: A model for research networking. Iran J Cult Health Promot 2024; 7 (4) :513-521.
11. Guidotti TL. The observatory: A model for studies in health, society, and the environment. J Environ Stud Sci (Internet). 2022;12(4):827–37.
DOI:10.1007/s13412-022-00786-6
12.Pooransingh S, Misir A, Ramdath D, Ramsewak S, Jaglal S, Cameron C, et al. Barriers and facilitators to establishing a national public health observatory. Rev Panam Salud Publica/Pan Am J Public Heal. 2015;38(5):403–9.
13. Damari B, Heidari A, Rashidian A, Vosoogh Moghaddam A, Khosravi A, Alikhani S. Designing a health observatory system for the Islamic Republic of Iran. Payesh 2020; 19 (5) :499-509.
14. Pourmalek F. National health observatories: Need for stepped-up action. The Health. 2012;3(3):63–4.
15. Barcellos C, Roux E, Ceccato P, Gosselin P, Monteiro AM, De Matos VP, et al. An observatory to gather and disseminate information on the health-related effects of environmental and climate change. Rev Panam Salud Publica/Pan Am J Public Heal. 2016;40(3):167–73.
16. Madela-Mntla EN, Jeenah M, Loots G, Mayosi BM. The development of a national health research observatory in south africa: Considerations and challenges. South African Heal Rev. 2016;2016(1): 235–41.
17. Varela AR, Hallal PC, Grueso JM, Pedišić Ž, Salvo D, Nguyen A, et al. Status and trends of physical activity surveillance, policy, and research in 164 countries: findings from the global observatory for physical activity—gopa! 2015 and 2020 surveys. J Phys Act Heal. 2023;20(2):112–28.
18. Milton K, Cavill N, Chalkley A, Foster C, Gomersall S, Hagstromer M, et al. Eight investments that work for physical activity. J Phys Act Heal. 2021;18(6):625–30.
19. Mina MJ, Metcalf CJE, McDermott AB, Douek DC, Farrar J, Grenfell BT. A global lmmunological observatory to meet a time of pandemics. Elife. 2020;9:1–5.
20. Mehrolhassani M, Amiresmaili M, Iranmanesh M. An evaluation model for monitoring human resources in the health system of iran . Irje. 2019;14 :40-9.
21. Farzadi F, Montazeri A, Sadighi J, Aeenparast A, Tavousi M, Maftoon F, et al. Observation of the implementation of the article 11 of general health policies in iran: the study protocol. Iran J Cult Health Promot. 2019;2(3):326-32.
22. Dias MA de S, Friche AA de L, Oliveira VB de, Caiaffa WT. The belo horizonte observatory for urban health: its history and current challenges. Cad Saude Publica. 2015;31(suppl 1):277–85.
23. Gigantesco A, Giuliani M, Graziano S, Zaami S, Tittarelli R, Pichini S, et al. The complex and constantly evolving public health threat of new psy. Ann Ist Super Sanità. 2011;47(4):363–72.
24. Røttingen JA, Regmi S, Eide M, Young AJ, Viergever RF, Ardal C, et al. Mapping of available health research and development data: what’s there, what’s missing, and what role is there for a global observatory? Lancet (Internet). 2013;382(9900):1286–307.
DOI:10.1016/S0140-6736(13)61046-6
25.Varela AR, Pratt M, Powell K, Lee IM, Bauman A, Heath G, et al. Worldwide surveillance, policy, and research on physical activity and health: The global observatory for physical activity. J Phys Act Heal. 2017;14(9):701–9.
26.Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global health workforce labor market projections for 2030. Hum Resour Health. 2017;15(1):1–12.
27. Zaveri A, Lehmann J, Auer S, Hassan MM, Sherif MA, Martin M. Publishing and interlinking the global health observatory dataset. Semant Web. 2013;4(3): 315–22.
28. Ramirez Varela A, Salvo D, Pratt M, Milton K, Siefken K, Bauman A, et al. Worldwide use of the first set of physical activity Country Cards: The Global Observatory for Physical Activity - GoPA! Int J Behav Nutr Phys Act. 2018;15(1):1–14.
29. Onagbiye S, Ricci H, Bester P, Ricci C. Sedentariness and overweight in relation to mortality in sub-Saharan Africa. A mediation analysis based on the World Health Organization-Global Health Observatory data repository. J Public Health Africa. 2023;14(4):71–6.
30. Li C, He WQ. Comparison of primary liver cancer mortality estimates from World Health Organization, global burden disease and global cancer observatory. Liver Int. 2022;42(10):2299–316.
31. Healy JM, Tang S, Patcharanarumol W, Annear PL.
A framework for comparative analysis of health systems: experiences from the Asia Pacific observatory on health systems and policies. WHO South-East Asia J public Heal. 2018;7(1):5–12.
Type of Study: Review Article |
Subject:
General
Received: 2025/09/6 | Accepted: 2026/04/30 | Published: 2026/06/1
Received: 2025/09/6 | Accepted: 2026/04/30 | Published: 2026/06/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
