

Volume 1, Issue 3 (9-2017)
EBHPME 2017, 1(3): 128-130 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Emamgholipour S. The Burden of Elderly’s Non-Communicable Diseases in Iran. EBHPME 2017; 1 (3) :128-130
URL: http://jebhpme.ssu.ac.ir/article-1-84-en.html
URL: http://jebhpme.ssu.ac.ir/article-1-84-en.html


Department of Health Management & Economics, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
Full-Text [PDF 269 kb]
(1549 Downloads)
| Abstract (HTML) (2700 Views)
Citation
This paper should be cited as: Emamgholipour S. The Burden of Elderly’s Non-Communicable Diseases in Iran. Evidence Based Health Policy, Management & Economics. 2017; 1(3): 128-30.
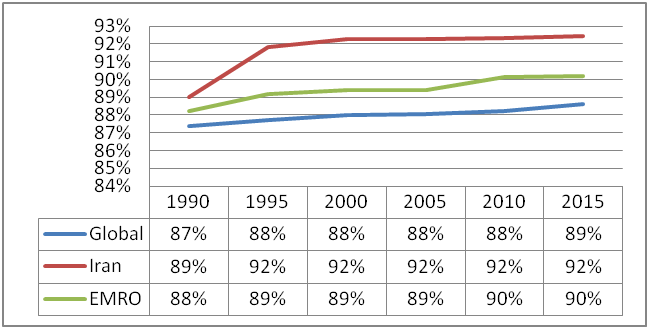
Figure 1. Percentage of total DALYs from NCDs in both genders, 70 + years
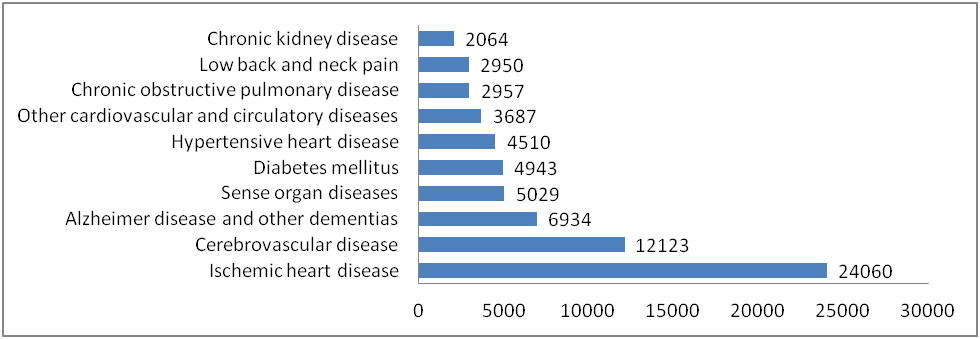
Figure 2. DALYs per 100,000 for 70 + years (3)
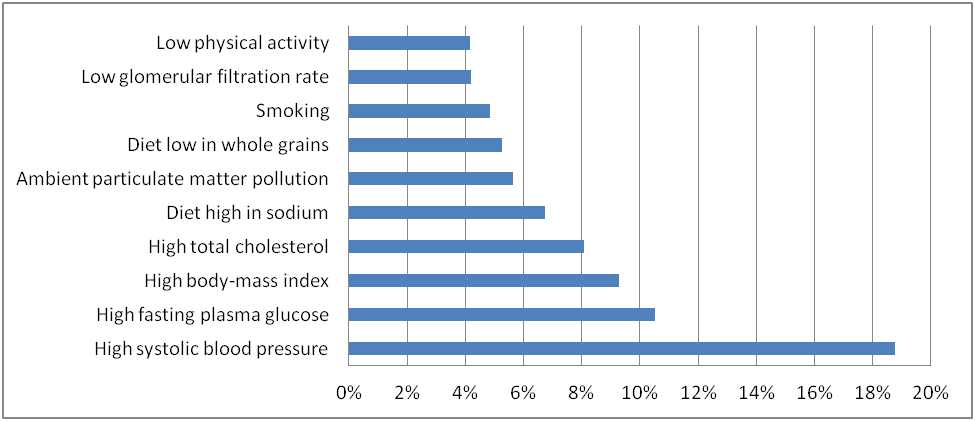
Figure 3. Ten major NCDs' risk factors attributed to with the highest share in DALYs in 70 + years
References
Full-Text: (1189 Views)
The Burden of Elderly’s Non-Communicable Diseases in Iran
Sara Emamgholipour
Department of Health Management & Economics Department, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
Sara Emamgholipour
Department of Health Management & Economics Department, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
| A R T I C L E I N F O | |
| Article History: Received: 7 Jun 2017 Revised: 9 Aug 2017 Accepted: 13 Sep 2017 |
|
| *Corresponding Author: Sara Emamgholipour Department of Health Management & Economics, School of Public Health, Tehran University of Medical Sciences, Poursina St., Qods St., Tehran, Iran. Email: s-emamgholipour@tums.ac.ir Tel: +98- 21- 42933240 |
|
Citation
This paper should be cited as: Emamgholipour S. The Burden of Elderly’s Non-Communicable Diseases in Iran. Evidence Based Health Policy, Management & Economics. 2017; 1(3): 128-30.
| A |
ll diseases can be examined in three groups with regard to disability and mortality burden: 1. Non-Communicable Diseases (NCDs), 2. Communicable diseases, congenital diseases, infant diseases, accidents and 3. injuries. Non-Communicable Diseases are the main causes of mortality and disability in the world. The World Economic Forum (WEF) estimates that NCDs will result in a global economic loss by US $ 47 trillion or 5% of the world Gross Domestic Product (GDP) during 2011-2030. In this regard, cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes may account for US $30 trillion loss (1). This figure will be higher if the individuals' utility loss due to diseases is accounted for. The ratio of Disability-Adjusted Life Years (DALYs) for people 65 + to total DALYs generated by NCDs among all age groups was 25% in 2015. Non-Communicable Diseases are avoidable through low-cost preventive health interventions. The experiences of highly developed countries show that decreasing the Risk Factors (RFs) rather than the medical cares can reduce the mortality rates originating from NCDs. In this way, a three-dollar return can be expected for one-dollar investment in preventing NCDs. Obviously, more recent medical interventions reported up to 10-fold more benefits (2). The burden of NCDs can be analyzed in two phases: first, this group of diseases may reduce the longevity and increase the mortality among all age groups; second, they can affect Quality of Life (QoL) and reduce it.
Figure 1. Percentage of total DALYs from NCDs in both genders, 70 + years
As Figure 1 shows, the share of NCDs burden from total diseases for all aged people (70 + years) in Iran was about 90-92% from 1990 to 2015. This ratio is higher than regional and world figures. It means that the elderly’s disability ratio generated by this group of diseases is higher in Iran than EMRO region and the world, on average. Figure 2, further shows ten top NCDs creating the highest disability ratios in terms of mortality and reduced QoL in 2015. The ischemic heart diseases got the first rank by 24,000 lives lost per 100,000 aged people.
Figure 2. DALYs per 100,000 for 70 + years (3)
The risk factors causing death and disability from NCDs are divided into three categories
of behavioral, metabolic, and environmental/ occupational. The most frequent disabilities among elderly people resulted from NCDs are attributed to behavioral and metabolic risk factors.
In more details, Figure 3 shows that high systolic blood pressure, high fasting plasma sugar, high BMI, high total cholesterol, diet high in sodium, ambient particulate matter pollution, diet low in whole grains, smoking, low glomerular filtration rate, and low physical activity are the 10 main factors in ascending order, which make the highest burden of diseases from NCDs in old people.
of behavioral, metabolic, and environmental/ occupational. The most frequent disabilities among elderly people resulted from NCDs are attributed to behavioral and metabolic risk factors.
In more details, Figure 3 shows that high systolic blood pressure, high fasting plasma sugar, high BMI, high total cholesterol, diet high in sodium, ambient particulate matter pollution, diet low in whole grains, smoking, low glomerular filtration rate, and low physical activity are the 10 main factors in ascending order, which make the highest burden of diseases from NCDs in old people.
Figure 3. Ten major NCDs' risk factors attributed to with the highest share in DALYs in 70 + years
Conclusion and discussion
Based on the results of the current study, the burden of NCDs in the elderly people of Iran is higher than that of the world and EMRO region, which in turn results in high expenditure for the Iranian health system. The most common causes of disability created by these diseases are the behavioral and metabolic risk factors originating from the individuals' lifestyle.
Ford and Capewell (2011) stated that in United State and high-income countries, reduction in risk factors and access to treatment result in respectively 44-76% and 23-37% decrease in mortality from heart disease.
In addition to conduction of interventions, the existence of an integrated health system can greatly reduce risk factors, especially metabolic risk factors in prevention, notification, and control phases (4).
Evidences from South Africa (5) and Iran (6) show that non-medical health staffs can also effectively control diabetes and high blood pressure.
Since lifestyle is the most important factor affecting NCDs, a targeted low cost policy can reduce their economic burden. Therefore, chronic diseases' management requires a comprehensive prevention program and should promote the social and health literacy of the population in a way that encourages people to have a healthier life style.
Moreover, population-based interventions such as increasing taxes on harmful commodities such as alcohol and tobacco, reducing salt intake and saturated fats, removing trans fatty acids from foods, reducing consumption of processed meat, informing people through the media, as well as conducting screening tests and drug treatments for high-risk people can be effective in this regard.
Based on the results of the current study, the burden of NCDs in the elderly people of Iran is higher than that of the world and EMRO region, which in turn results in high expenditure for the Iranian health system. The most common causes of disability created by these diseases are the behavioral and metabolic risk factors originating from the individuals' lifestyle.
Ford and Capewell (2011) stated that in United State and high-income countries, reduction in risk factors and access to treatment result in respectively 44-76% and 23-37% decrease in mortality from heart disease.
In addition to conduction of interventions, the existence of an integrated health system can greatly reduce risk factors, especially metabolic risk factors in prevention, notification, and control phases (4).
Evidences from South Africa (5) and Iran (6) show that non-medical health staffs can also effectively control diabetes and high blood pressure.
Since lifestyle is the most important factor affecting NCDs, a targeted low cost policy can reduce their economic burden. Therefore, chronic diseases' management requires a comprehensive prevention program and should promote the social and health literacy of the population in a way that encourages people to have a healthier life style.
Moreover, population-based interventions such as increasing taxes on harmful commodities such as alcohol and tobacco, reducing salt intake and saturated fats, removing trans fatty acids from foods, reducing consumption of processed meat, informing people through the media, as well as conducting screening tests and drug treatments for high-risk people can be effective in this regard.
References
1) Hunter DJ, Reddy KS. Noncommunicable diseases. New England Journal of Medicine. 2013; 369(14): 1336-43.
2) Chand S. Silent killer, economic opportunity: rethinking non-communicable disease: Chatham House; 2012. Available from URL: www. chathamhouse. org.
3) Global burden of disease. Available from URL: www.WHO.int.
4) Ford ES, Capewell S. Proportion of the decline in cardiovascular mortality disease due to prevention versus treatment: public health versus clinical care. Annual Review of Public Health. 2011; 32: 5-22.
5) Coleman R, Gill G, Wilkinson D. Noncommunicable disease management in resource-poor settings: a primary care model from rural South Africa. Bulletin of the World Health Organization. 1998; 76(6): 633.
6) Farzadfar F, Murray CJ, Gakidou E, Bossert T, Namdaritabar H, Alikhani S, et al. Effectiveness of diabetes and hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study. The Lancet. 2012; 379(9810): 47-54.
2) Chand S. Silent killer, economic opportunity: rethinking non-communicable disease: Chatham House; 2012. Available from URL: www. chathamhouse. org.
3) Global burden of disease. Available from URL: www.WHO.int.
4) Ford ES, Capewell S. Proportion of the decline in cardiovascular mortality disease due to prevention versus treatment: public health versus clinical care. Annual Review of Public Health. 2011; 32: 5-22.
5) Coleman R, Gill G, Wilkinson D. Noncommunicable disease management in resource-poor settings: a primary care model from rural South Africa. Bulletin of the World Health Organization. 1998; 76(6): 633.
6) Farzadfar F, Murray CJ, Gakidou E, Bossert T, Namdaritabar H, Alikhani S, et al. Effectiveness of diabetes and hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study. The Lancet. 2012; 379(9810): 47-54.
Type of Study: Letter to Editor |
Subject:
Health Policy
Received: 2017/06/7 | Accepted: 2017/09/13 | Published: 2018/03/17
Received: 2017/06/7 | Accepted: 2017/09/13 | Published: 2018/03/17
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
