

Volume 6, Issue 3 (10-2022)
EBHPME 2022, 6(3): 207-216 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Niazi M, Zolfaghari A, Vahedian M, Mahdian A. Meta-Analysis of Studies on the Effects of Rehabilitation on the Quality of Life in Patients with Heart Diseases in Iran from 2007 to 2017. EBHPME 2022; 6 (3) :207-216
URL: http://jebhpme.ssu.ac.ir/article-1-368-en.html
URL: http://jebhpme.ssu.ac.ir/article-1-368-en.html



Department of Political Science, Faculty of Social Sciences, Payame Noor University, Tehran, Iran , akbarzolfaghari@pnu.ac.ir
Full-Text [PDF 655 kb]
(595 Downloads)
| Abstract (HTML) (1590 Views)
Full-Text: (228 Views)
Background: Heart disease is one of the most common types of diseases in the contemporary world. In the treatment process, rehabilitation programs can bring patients back to the course of daily life as soon as possible, and improve their functional levels life quality. The present study used the meta-analysis method on studies that have examined the effects of rehabilitation on the life quality of heart patients.
Methods: Based on meta-analysis method, the researchers tried to compile different studies conducted at different periods in the form of a specific subject. Then, the research results were examined in a systematic way. The statistical population of this study included all the scientific and research papers on the effects of rehabilitation programs regarding the life quality of heart patients. They were studies from 2007 to the end of 2017 published in scientific journals. 44 studies regarding the life quality of heart patients have been conducted. Finally, 10 studies were selected as a sample and meta-analysis was performed using the Comprehensive Meta-Analysis Software 2(CMA2).
Results: Results of the study demonstrate that all the studies on the effects of rehabilitation on life quality of heart patients were significant. This means that the relationship between the variables considered in each study was statistically related, and this relationship was correct.
Conclusion: It is concluded that sports rehabilitation has the highest impact on life quality and physical and mental dimensions. Generally, all effects’ sizes are significant. This confirms that the results of all the research conducted regarding the effect of rehabilitation programs on the life quality of heart patients are correct; rehabilitation has an effect on improving the quality of life.
Key words: Quality of Life, Heart disease, Rehabilitation, Meta-analysis.
Materials and Methods
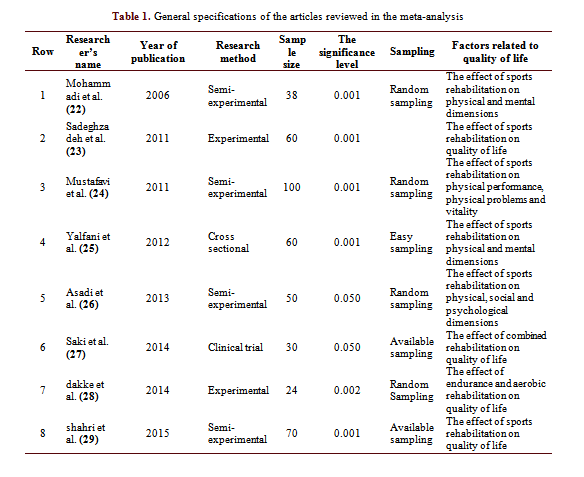
Based on the meta-analysis method, the researchers tried to compile different studies that have been done at different periods of time in the form of a specific subject. This is followed by examining the research results in a systematic format. The basis of meta-analysis method is that the unit of analysis is taken from the study, not the subject(21). This is until the combined secondary analysis finally reveals the information that the primary analysis does not. Using meta-analysis method, this study has reviewed all the studies conducted in the field of heart disease. Based on the appropriate criteria in meta-analysis, studies related to the research topic had been selected. Accordingly, the statistical population of the present study was all studies conducted in the field of rehabilitation effects of heart disease in the period from 2007 to 2017. Exercise testing, quality of life questionnaires, especially the standard McNew quality of life questionnaire, were the most important tools for measuring life quality in the studies regarding social, physical, mental and psychological dimensions. The keywords used for the search were ‘heart disease, quality of life of heart patients, rehabilitation of heart patients’ in Persian. They were indexed in one of the scientific databases of the Jahad Daneshgahi University (SID), Noor Specialized Journals (Noormags), the country's publications (Magiran), Iranian scientific documentation center (Irandoc). Semi-experimental, experimental, cross-sectional and clinical trials were the types of studies used in this study. 44 papers were found in this field, 10 of which were selected for meta-analysis. The method has 5 stages: 1. Asking questions, 2. Searching for literature, 3. Selecting qualified research, 4. Data extraction and evaluating its quality and validity, and 5. Composing, interpreting and interpreting the report. The studies included in the meta-analysis are mentioned in Table 1.
Selection of studies
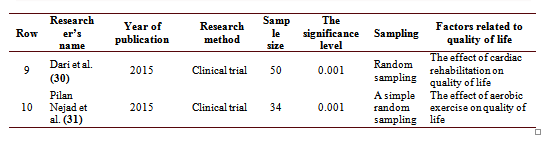
In this research, the studies have been selected in the following order: 1- The research has been done in Persian language. 2- In the relevant study, two issues of rehabilitation and quality of life have been analyzed. 3- The study has provided the statistical information required for practical extraction of the size of the sample. Figure 1 lists the inclusion and exclusion criteria for meta-analysis studies. The selected studies were analyzed using CMA version 2 software.
Discussion
Most patients with heart valve surgery continue to suffer from heart failure and inability to perform daily tasks after surgery. Cardiac rehabilitation is an effective way to reduce the complications of heart surgery. The results of research in this field indicate that patients who receive rehabilitation services after surgery show improved vitality and condition in different dimensions of life quality, including physical, mental and social.
In the context, the research of Schönfelder et al. (33) shows that in sum, 6 weeks of exercise-based outpatient cardiac rehabilitation significantly improves not only physical work capacity but also quality of life. Whereas, the research of Zahedi and Shirmohammadi (34), showed that the implementation of an exercise-based cardiac rehabilitation program improves left ventricular function in patients with myocardial infarction after primary PCI but does not affect right ventricular function. It shows that cardiac rehabilitation program may be associated with the gender and the age of the patients. Of course, it should be noted that clinicians, health care leaders, and payers should show attention to incorporating CR as part of standard care for patients with HF (35). Also, some studies admit that about the accuracy of rehabilitation rates; additional long-term studies assessing safety, adherence, and morbidity and mortality are required before high-intensity CR training can be more widely recommended, especially in previously sedentary patients with known or suspected CVD exercising in non-medically supervised settings(36). Finally, it should be said that studies related to this field suggest different issues in the field of rehabilitation, such as the study by Kikuchi et al(37), suggests that home-based CR using an integrated telerehabilitation platform may be a potential option for patients who are unable to participate in center-based CR due to geographic or social accessibility and physical barrier issues. Franklin and Quindry (36), believe that moderate intensity swimming exercise might improve the right ventricular remodeling by regulating the levels of GLS
Conclusion
In this study, the meta-analysis method was used and a systematic approach was adopted regarding the studies on the effects of rehabilitation programs on the quality of life of heart patients. On the one hand, the effect of different practical and experimental studies was specified. On the other hand, the average size of the effects of the entire research was determined.
Based on the data in Table 4, the results of the homogeneity and heterogeneity tests are equal to Q = 5.954 and P-value = 0.744. The P-value over 0.050 confirms the null hypothesis, indicating studies regarding the effect of rehabilitation on the life quality of heart patients are homogeneous. Given that the I2 index coefficient is close to zero, it can be said that studies in this area are highly homogeneous.
This means that sports rehabilitation has the highest impact on life quality and physical and mental dimensions. In general, all size effects are significant. This suggests that the results of all studies conducted regarding the effect of rehabilitation programs on the life quality heart patients are correct.
Acknowledgments
We would like to appreciate the experts and professors who helped us to identify original papers and keywords.
Conflict of interests
The authors declared no conflict of interests.
Authors' Contributions
Mohsen Niazi, Akbar Zolfaghari, Morteza Vahedian, and Aida Mahdian designed research, Mohsen Niazi, Akbar Zolfaghari, Morteza Vahedian, and Aida Mahdian conducted research, Mohsen Niazi, Akbar Zolfaghari, Morteza Vahedian, and Aida Mahdian analyzed data, and wrote the paper and have primary responsibility for the final content. All authors read and approved the final manuscript.
Funding
The authors declared no conflict of interests.
Methods: Based on meta-analysis method, the researchers tried to compile different studies conducted at different periods in the form of a specific subject. Then, the research results were examined in a systematic way. The statistical population of this study included all the scientific and research papers on the effects of rehabilitation programs regarding the life quality of heart patients. They were studies from 2007 to the end of 2017 published in scientific journals. 44 studies regarding the life quality of heart patients have been conducted. Finally, 10 studies were selected as a sample and meta-analysis was performed using the Comprehensive Meta-Analysis Software 2(CMA2).
Results: Results of the study demonstrate that all the studies on the effects of rehabilitation on life quality of heart patients were significant. This means that the relationship between the variables considered in each study was statistically related, and this relationship was correct.
Conclusion: It is concluded that sports rehabilitation has the highest impact on life quality and physical and mental dimensions. Generally, all effects’ sizes are significant. This confirms that the results of all the research conducted regarding the effect of rehabilitation programs on the life quality of heart patients are correct; rehabilitation has an effect on improving the quality of life.
Key words: Quality of Life, Heart disease, Rehabilitation, Meta-analysis.
Introduction
Heart failure is one of the most important causes of death in the industrialized world and developed countries (1). It is also one of the main obstacles regarding physical activity (2). This restriction is directly related to the activities of daily life and the lifestyle changes imposed by the disease (3). Hence, it reduces the quality of life (3, 4). Quality of life is a concept related to interdisciplinary approaches including medicine, sociology, psychology, economics and philosophy. This concept is very important among heart patients because it predicts death after hospital discharge (5). Among the things that improve the life quality and level of physical activity a heart patient, are rehabilitation therapies. In addition to preventing the progression of the disease, one of the important goals of rehabilitation is improving the life quality of the patient (6). Recovery from heart disease deals with a set of required activities used to positively affect the physical, mental and social condition of the patient (7). Therefore, exercising is an integral part of this paradigm (8, 9).
Many studies have demonstrated that cardiac rehabilitation improves disease-related symptoms, quality of life, and clinical outcomes. Exercise is prescribed to reduce fatigue and shortness of breath (10). Moreover, exercise in patients with heart failure is associated with improvement in physical activities of daily life, anxiety, depression and general well-being, according to the results of studies (11). Traditional methods of rehabilitation focus on aerobic exercise (8, 12). In patients with heart failure, however, exercise capacity may be limited by a number of frequently associated factors such as decreased contraction, diastolic dysfunction, chronotropic insufficiency, oxygen metabolism, or skeletal muscle mass. At the peak of exercise, heart should increase cardiac output, and diastolic mechanisms should be adjusted by reducing the time. Patients with heart failure may not be able to achieve this essential increase in diastolic relaxation in order to increase preload (13). However, it is now accepted that exercise intolerance in heart patients is not solely due to central cardiovascular factors, and as a result, physicians go beyond that. Based on the "Muscle Hypothesis", the central treatment method specifically argues that those abnormalities begin in the peripheral muscle tissue and form disease progression (14). This approach argues that targeting muscle disorders may disrupt these maladaptive feedback loops and improve exercise tolerance (15). As a result, exercise has been accepted as a treatment for patients and is beneficial in terms of improving mortality, life quality and functionality (16–18). In this regard, previous studies suggest a significant improvement in all aspects of life quality after a comprehensive cardiac rehabilitation program for patients with chronic and non-ischemic failure (16, 19). On the other hand, reducing exercise is a major factor which limits the daily lives of patients with chronic heart failure. Thus, it destroys their quality of life (20). This paper intends to review studies regarding rehabilitation of heart patients in the country to determine their effect using meta-analysis.Materials and Methods
Based on the meta-analysis method, the researchers tried to compile different studies that have been done at different periods of time in the form of a specific subject. This is followed by examining the research results in a systematic format. The basis of meta-analysis method is that the unit of analysis is taken from the study, not the subject(21). This is until the combined secondary analysis finally reveals the information that the primary analysis does not. Using meta-analysis method, this study has reviewed all the studies conducted in the field of heart disease. Based on the appropriate criteria in meta-analysis, studies related to the research topic had been selected. Accordingly, the statistical population of the present study was all studies conducted in the field of rehabilitation effects of heart disease in the period from 2007 to 2017. Exercise testing, quality of life questionnaires, especially the standard McNew quality of life questionnaire, were the most important tools for measuring life quality in the studies regarding social, physical, mental and psychological dimensions. The keywords used for the search were ‘heart disease, quality of life of heart patients, rehabilitation of heart patients’ in Persian. They were indexed in one of the scientific databases of the Jahad Daneshgahi University (SID), Noor Specialized Journals (Noormags), the country's publications (Magiran), Iranian scientific documentation center (Irandoc). Semi-experimental, experimental, cross-sectional and clinical trials were the types of studies used in this study. 44 papers were found in this field, 10 of which were selected for meta-analysis. The method has 5 stages: 1. Asking questions, 2. Searching for literature, 3. Selecting qualified research, 4. Data extraction and evaluating its quality and validity, and 5. Composing, interpreting and interpreting the report. The studies included in the meta-analysis are mentioned in Table 1.
Selection of studies
In this research, the studies have been selected in the following order: 1- The research has been done in Persian language. 2- In the relevant study, two issues of rehabilitation and quality of life have been analyzed. 3- The study has provided the statistical information required for practical extraction of the size of the sample. Figure 1 lists the inclusion and exclusion criteria for meta-analysis studies. The selected studies were analyzed using CMA version 2 software.
Results
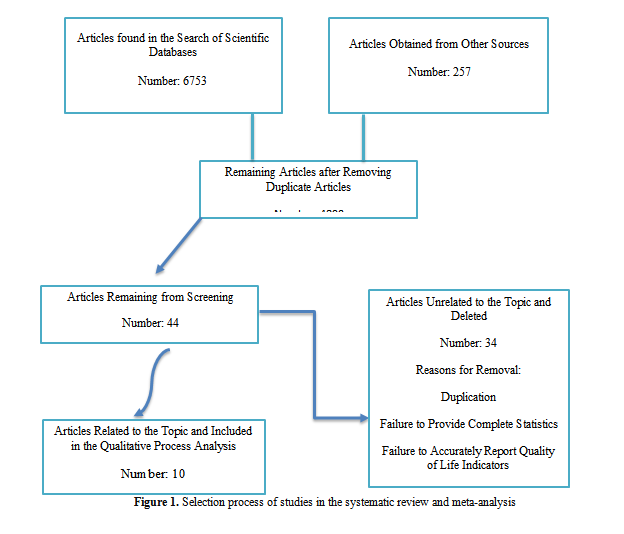
This paper intends to review studies regarding rehabilitation of heart patients in the country to determine their effect using meta-analysis. The size of effect in the meta-analysis method indicates the weight and effect of each study. In other words, the value of the size of work indicates which research results have the greatest impact on studies in that field. By the size of the effect, the researcher finds out how much the independent variables have affected the dependent variable. To interpret the size obtained through reviewing the history of social research, the researcher has calculated the size of the study. Then, it would be averaged as a suitable criterion for comparing other sizes (32).
The data in Table 2 demonstrates that all the studies on the effects of rehabilitation on life quality of heart patients were significant. This means that the relationship between the variables considered in each study was statistically related, and this relationship is correct. Based on Table 3, Dekeh et al (28) ’s research, with a rate of 0.599, followed by Dori et al (30) 's research with a rate of 0.522, and Mohammadi et al. (22) with an effect size of 0.513, have the highest impact among the 10 studies conducted in this field.
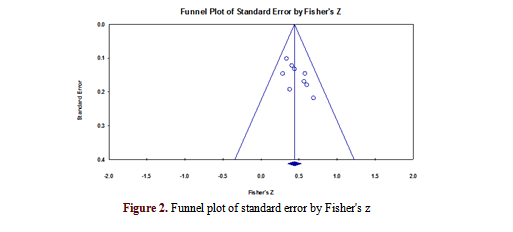
Release bias: Dissemination bias means that the final results and estimates of the research are biased and erroneous. Based on the propagation error, the researcher can find out how reliable the results of the meta-analysis are. Generally, the publication error occurs due to the weakness of the research or the omission of the results of a research in meta-analysis. There are various methods for measuring propagation error. The most common one is the use of a funnel diagram. The results of the funnel diagram are interpreted in such a way that the closer the studies are to the top of the funnel, the less propagation error there is. In addition to the funnel diagram in this study, the Beck and Mesomorphic rank correlation method and N safe from error have been used. The results of these methods are presented in the following sections.
Funnel diagram
The following is a funnel diagram of the studies in the present research, in order to investigate the propagation error in the following section. As the funnel diagram shows, most of the studies are at the top of the funnel, and there is a relative symmetry between the dispersion of studies. In general, the above funnel diagram indicates that there is no error in publishing the studies of this meta-analysis.
The Beck and Mesomorphic Rank Correlations Results
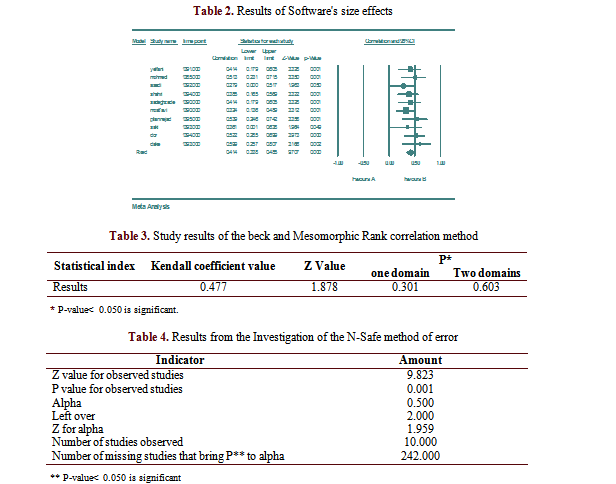
If the significance level of the Beck and Mesomorphic test is greater than 0.050, the authors can conclude that there is no publication bias. P value in the table above is 0.603 in two ranges and 0.301 in one range. These values are more than 0.050. Therefore, the assumption of no bias of the diffusion is confirmed.
N safe results from error
The Error-Free N-Test is interpreted regarding the basis. If a number of studies are required to challenge the results of the meta-analysis, the research has a diffusion error. The results of this test are presented below in Table 4.
The results of Table 4 indicate that if 242 more studies are conducted in this area, the value of the combined bilateral P-value will not exceed 0.050. This means that another 242 studies must be conducted to cast doubt on the current research estimates. Q test was used to evaluate the homogeneity of the studies.
Based on the data in Table 4, the results of the homogeneity and heterogeneity tests are equal to Q = 5.954 and P-value = 0.744. The P-value over 0.050 confirms the null hypothesis, indicating studies regarding the effect of rehabilitation on the life quality of heart patients are homogeneous. Given that the I2 index coefficient is close to zero, it can be said that studies in this area are highly homogeneous.
This paper intends to review studies regarding rehabilitation of heart patients in the country to determine their effect using meta-analysis. The size of effect in the meta-analysis method indicates the weight and effect of each study. In other words, the value of the size of work indicates which research results have the greatest impact on studies in that field. By the size of the effect, the researcher finds out how much the independent variables have affected the dependent variable. To interpret the size obtained through reviewing the history of social research, the researcher has calculated the size of the study. Then, it would be averaged as a suitable criterion for comparing other sizes (32).
The data in Table 2 demonstrates that all the studies on the effects of rehabilitation on life quality of heart patients were significant. This means that the relationship between the variables considered in each study was statistically related, and this relationship is correct. Based on Table 3, Dekeh et al (28) ’s research, with a rate of 0.599, followed by Dori et al (30) 's research with a rate of 0.522, and Mohammadi et al. (22) with an effect size of 0.513, have the highest impact among the 10 studies conducted in this field.
Release bias: Dissemination bias means that the final results and estimates of the research are biased and erroneous. Based on the propagation error, the researcher can find out how reliable the results of the meta-analysis are. Generally, the publication error occurs due to the weakness of the research or the omission of the results of a research in meta-analysis. There are various methods for measuring propagation error. The most common one is the use of a funnel diagram. The results of the funnel diagram are interpreted in such a way that the closer the studies are to the top of the funnel, the less propagation error there is. In addition to the funnel diagram in this study, the Beck and Mesomorphic rank correlation method and N safe from error have been used. The results of these methods are presented in the following sections.
Funnel diagram
The following is a funnel diagram of the studies in the present research, in order to investigate the propagation error in the following section. As the funnel diagram shows, most of the studies are at the top of the funnel, and there is a relative symmetry between the dispersion of studies. In general, the above funnel diagram indicates that there is no error in publishing the studies of this meta-analysis.
The Beck and Mesomorphic Rank Correlations Results
If the significance level of the Beck and Mesomorphic test is greater than 0.050, the authors can conclude that there is no publication bias. P value in the table above is 0.603 in two ranges and 0.301 in one range. These values are more than 0.050. Therefore, the assumption of no bias of the diffusion is confirmed.
N safe results from error
The Error-Free N-Test is interpreted regarding the basis. If a number of studies are required to challenge the results of the meta-analysis, the research has a diffusion error. The results of this test are presented below in Table 4.
The results of Table 4 indicate that if 242 more studies are conducted in this area, the value of the combined bilateral P-value will not exceed 0.050. This means that another 242 studies must be conducted to cast doubt on the current research estimates. Q test was used to evaluate the homogeneity of the studies.
Based on the data in Table 4, the results of the homogeneity and heterogeneity tests are equal to Q = 5.954 and P-value = 0.744. The P-value over 0.050 confirms the null hypothesis, indicating studies regarding the effect of rehabilitation on the life quality of heart patients are homogeneous. Given that the I2 index coefficient is close to zero, it can be said that studies in this area are highly homogeneous.
Discussion
Most patients with heart valve surgery continue to suffer from heart failure and inability to perform daily tasks after surgery. Cardiac rehabilitation is an effective way to reduce the complications of heart surgery. The results of research in this field indicate that patients who receive rehabilitation services after surgery show improved vitality and condition in different dimensions of life quality, including physical, mental and social.
In the context, the research of Schönfelder et al. (33) shows that in sum, 6 weeks of exercise-based outpatient cardiac rehabilitation significantly improves not only physical work capacity but also quality of life. Whereas, the research of Zahedi and Shirmohammadi (34), showed that the implementation of an exercise-based cardiac rehabilitation program improves left ventricular function in patients with myocardial infarction after primary PCI but does not affect right ventricular function. It shows that cardiac rehabilitation program may be associated with the gender and the age of the patients. Of course, it should be noted that clinicians, health care leaders, and payers should show attention to incorporating CR as part of standard care for patients with HF (35). Also, some studies admit that about the accuracy of rehabilitation rates; additional long-term studies assessing safety, adherence, and morbidity and mortality are required before high-intensity CR training can be more widely recommended, especially in previously sedentary patients with known or suspected CVD exercising in non-medically supervised settings(36). Finally, it should be said that studies related to this field suggest different issues in the field of rehabilitation, such as the study by Kikuchi et al(37), suggests that home-based CR using an integrated telerehabilitation platform may be a potential option for patients who are unable to participate in center-based CR due to geographic or social accessibility and physical barrier issues. Franklin and Quindry (36), believe that moderate intensity swimming exercise might improve the right ventricular remodeling by regulating the levels of GLS
Conclusion
In this study, the meta-analysis method was used and a systematic approach was adopted regarding the studies on the effects of rehabilitation programs on the quality of life of heart patients. On the one hand, the effect of different practical and experimental studies was specified. On the other hand, the average size of the effects of the entire research was determined.
Based on the data in Table 4, the results of the homogeneity and heterogeneity tests are equal to Q = 5.954 and P-value = 0.744. The P-value over 0.050 confirms the null hypothesis, indicating studies regarding the effect of rehabilitation on the life quality of heart patients are homogeneous. Given that the I2 index coefficient is close to zero, it can be said that studies in this area are highly homogeneous.
This means that sports rehabilitation has the highest impact on life quality and physical and mental dimensions. In general, all size effects are significant. This suggests that the results of all studies conducted regarding the effect of rehabilitation programs on the life quality heart patients are correct.
Acknowledgments
We would like to appreciate the experts and professors who helped us to identify original papers and keywords.
Conflict of interests
The authors declared no conflict of interests.
Authors' Contributions
Mohsen Niazi, Akbar Zolfaghari, Morteza Vahedian, and Aida Mahdian designed research, Mohsen Niazi, Akbar Zolfaghari, Morteza Vahedian, and Aida Mahdian conducted research, Mohsen Niazi, Akbar Zolfaghari, Morteza Vahedian, and Aida Mahdian analyzed data, and wrote the paper and have primary responsibility for the final content. All authors read and approved the final manuscript.
Funding
The authors declared no conflict of interests.
Type of Study: Review Article |
Subject:
General
Received: 2021/11/22 | Accepted: 2022/10/18 | Published: 2022/10/18
Received: 2021/11/22 | Accepted: 2022/10/18 | Published: 2022/10/18
References
1. Fonarow GC, Adams KF, Abraham WT, Yancy CW, Boscardin WJ, ADHERE Scientific Advisory Committee. Risk stratification for in-hospital mortality in acutely decompensated heart failure: Classification and regression tree analysis. Jama. 2005; 293(5): 572-80. [DOI: 10.1001/jama.293.5.572]
2. Santos JJA dos, Plewka JEA, Brofman PRS. Quality of life and clinical indicators in heart failure: A multivariate analysis. Arq Bras Cardiol. 2009; 93(2): 159-66. [DOI: 10.1590/s0066-782x2009000800015]
3. Malik FA, Gysels M, Higginson IJ. Living with breathlessness: A survey of caregivers of breathless patients with lung cancer or heart failure. Palliat Med. 2013; 27(7): 647-56. [DOI: 10.1177/0269216313488812]
4. Wilhelmsen L, Rosengren A, Eriksson H, Lappas G. Heart failure in the general population of men–morbidity, risk factors and prognosis. J Intern Med. 2001; 249(3): 253-61. [DOI: 10.1046/j.1365-2796.2001.00801.x]
5. Bowling CB, Fonarow GC, Patel K, Zhang Y, Feller MA, Sui X, et al. Impairment of activities of daily living and incident heart failure in community‐dwelling older adults. Eur J Heart Fail. 2012; 14(6): 581-7. [DOI: 10.1093/ eurjhf/hfs034]
6. Pihl E, Cider Å, Strömberg A, Fridlund B, Mårtensson J. Exercise in elderly patients with chronic heart failure in primary care: Effects on physical capacity and health-related quality of life. Eur J Cardiovasc Nurs. 2011; 10(3): 150-8. [DOI: 10.1016/j.ejcnurse.2011.03.002]
7. Jette M, Heller R, Landry F, Blümchen G. Randomized 4-week exercise program in patients with impaired left ventricular function. Circulation. 1991; 84(4): 1561-7. [DOI: 10.1161/ 01.cir.84.4.1561]
8. O’Connor ChM, Whellan DJ, Lee KL, Keteyian SJ, Cooper LS, Ellis SJ, et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. Jama. 2009; 301(14): 1439-50. [DOI: 10.1001/jama.2009.454]
9. Piña IL, Apstein CS, Balady GJ, Belardinelli R, Chaitman BR, Duscha BD, et al. Exercise and heart failure: A statement from the American Heart Association Committee on exercise, rehabilitation, and prevention. Circulation. 2003; 107(8): 1210-25. [DOI: 10.1161/01. cir. 0000055013.92097.40]
10. Giannuzzi P, Temporelli PL, Corrà U, Gattone M, Giordano A, Tavazzi L. Attenuation of unfavorable remodeling by exercise training in postinfarction patients with left ventricular dysfunction: Results of the Exercise in Left Ventricular Dysfunction (ELVD) trial. Circulation. 1997; 96(6): 1790-7. [DOI: 10.1161/01.cir.96.6.1790]
11. Kokkinos PF, Choucair W, Graves P, Papademetriou V, Ellahham S. Chronic heart failure and exercise. American Heart Journal. 2000; 140(1): 21-8. [DOI: 10.1067/mhj.2000.106916]
12. Coats AJ, Adamopoulos S, Meyer TE, Conway J, Sleight P. Effects of physical training in chronic heart failure. The Lancet. 1990; 335(8681): 63-6. [DOI: 10.1016/0140-6736(90)90536-e]
13. Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al. Executive summary: Heart disease and stroke statistics—2010 update. Circulation. 2010; 121(7): 948–54. [DOI: 10.1161/ CIRCULATIONAHA.109.192666]
14. Piepoli MF, Stewart Coats AJ. The ‘skeletal muscle hypothesis in heart failure’ revised. European Heart Journal. 2013; 34(7): 486-8. [DOI: 10.1093/eurheartj/ehs463]
15. Piepoli M, Clark AL, Volterrani M, Adamopoulos S, Sleight P, Coats AJ. Contribution of muscle afferents to the hemodynamic, autonomic, and ventilatory responses to exercise in patients with chronic heart failure: effects of physical training. Circulation. 1996; 93(5): 940-52. [DOI: 10.1161/01.cir.93.5.940]
16. Van Tol BA, Huijsmans RJ, Kroon DW, Schothorst M, Kwakkel G. Effects of exercise training on cardiac performance, exercise capacity and quality of life in patients with heart failure: a meta‐analysis. Eur J Heart Fail. 2006; 8(8): 841-50. [DOI: 10.1016/j.ejheart.2006.02.013]
17. Selig SE, Levinger I, Williams AD, Smart N, Holland DJ, Maiorana A, et al. Exercise & sports science Australia position statement on exercise training and chronic heart failure. J Sci Med Sport. 2010; 13(3): 288-94. [DOI: 10.1016/j.jsams.2010.01.004]
18. Schmid J-P, Blatter-Bühler P, Gaillet R, Binder RK, Walker Schmid R, Mohacsi P, et al. Impact of a cardiac rehabilitation programme on exercise capacity, parameters of left ventricular function and health related quality of life in chronic heart failure patients: Results from a prospective single centre cohort. Cardiovasc Med. 2010; 13: 86-91.
19. Sarullo FM, Gristina T, Brusca I, Milia S, Raimondi R, Sajeva M, et al. Effect of physical training on exercise capacity, gas exchange and N-terminal pro-brain natriuretic peptide levels in patients with chronic heart failure. Eur J Prev Cardiol. 2006; 13(5): 812-7. [DOI: 10.1097/ 01.hjr.0000238396.42718.61]
20. Smart N. Exercise training for heart failure patients with and without systolic dysfunction: An evidence-based analysis of how patients benefit. Cardiol Res Pract. 2011; 2011: 837238. [DOI: 10.4061/2011/837238]
21. Niazi M, Hosseinizadeh S, Sakhaei A. Meta-Analysis (Theory to Application). Tehran: Sokhanvaran; 2016. [In Persian]
22. Mohammadi F, Taherian A, Hosseini MA, Rahgozar M. Effect of home-based cardiac rehabilitation quality of life in the patients
with myocardical infarction. Archives of Rehabilitation. 2006; 7(3): 0-0. [In Persian]
23. Sadeghzadeh V, Moshtagh Eshgh Z. Effect of cardiac rehabilitation on quality of life in myocardial infarction patients in Zanjan. Advances in Nursing and Midwifery. 2011; 21(72): 8-13. [In Persian]
24. Saeidi M, Mostafavi S, Heidari H, Masoudi S. Effects of a comprehensive cardiac rehabilitation program on quality of life in patients with coronary artery disease. ARYA Atheroscler. 2013; 9(3): 179-85.
25. Yalfani A, Nazem F, Safiarian R, Jargeh M. The effects of exercise cardiac rehabilitation on anxiety, depression and quality of life in coronary artery bypass grafting patients. Avicenna Journal of Clinical Medicine. 2012;19(1): 39-44. [In Persian].
26. Makarem A, Asadi M, Mohammadi F, Hosseini MA. Effect of hospital based cardiac rehabilitation on quality of life of patients with myocardial infarction, Baghiatallah hospital, 2010. Arch Rehabil. 2013;14(3): 56-63. [In Persian]
27. Saki B, Ebrahim Kh, Abedi-Yekta A, Salehifard L, Malekipoor A, Hasabi M. The effect of the eight-week concurrent training on quality of life in patients with myocardial infarction. Iranian Journal of Cardiovascular Nursin. 2015; 3(4): 6-13. [In Persian]
28. Dakei Z, Hemmat Far A, Azizbeigi kamal and. Effect of resistance and endurance training protocols on functional capacity and quality of life in male patients after myocardial infarction. Iranian Journal of Cardiovascular Nursing. 2014; 3(1): 26-33. [In Persian]
29. Mahdavi Shahri SM, Abbasi I, Mohammadi N. Effect of cardiac rehabilitation program on quality of life in patients undergoing coronary artery bypass graft surgery. Quarterly of the Horizon of Medical Sciences. 2015; 21(2): 67-74.
30. Dorri S, khalifehzadeh Esfahani A, Dorri S. Quality of life and return to work after cardiac rehabilitation in acute coronary syndrome patients. Iranian Journal of Cardiovascular Nursing. 2015; 4(1): 48-57. [In Persian]
31. Pilannejad S, Naimi SS, Okhovatian F, Attarbashi Moghadam B, Jamalian SA, Akbarzadeh Bagheban A. The effect of the first phase of cardiac rehabilitation on quality of life and functional capacity of patients with heart failure. Scientific Journal of Rehabilitation Medicine. 2017; 6(2): 82-90. [In Persian] [DOI: 10.22037/ JRM.2017.1100306]
32. Tamim RM, Bernard RM, Borokhovski E, Abrami PC, Schmid RF. What forty years of research says about the impact of technology on learning: A second-order meta-analysis and validation study. Rev Educ Res. 2011; 81(1): 4-28. [DOI: 10.3102/0034654310393361]
33. Schönfelder M, Oberreiter H, Egger A, Tschentscher M, Droese S, Niebauer J. Effect of different endurance training protocols during cardiac rehabilitation on quality of life. Am J Med. 2021; 134(6): 805-11. [DOI: 10.1016/j.amjmed.2020.10.048]
34. Zahedi M, Shirmohammadi M. The effect of cardiac rehabilitation on left and right ventricular function in post primary PCI patients. Ann Med Surg. 2022; 79: 104093. [DOI: 10.1016/j. amsu.2022.104093]
35. Bozkurt B, Fonarow GC, Goldberg LR, Guglin M, Josephson RA, Forman DE, et al. Cardiac rehabilitation for patients with heart failure: JACC expert panel. J Am Coll Cardiol. 2021; 77(11): 1454-69. [DOI: 10.1016/j. jacc.2021.01.030]
36. Franklin BA, Quindry J. High level physical activity in cardiac rehabilitation: Implications for exercise training and leisure-time pursuits. Prog Cardiovasc Dis. 2022; 70: 22-32. [DOI: 10.1016/j.pcad.2021.12.005]
37. Kikuchi A, Taniguchi T, Nakamoto K, Sera F, Ohtani T, Yamada T, et al. Feasibility of home-based cardiac rehabilitation using an integrated telerehabilitation platform in elderly patients with heart failure: A pilot study. J Cardiol. 2021; 78(1): 66-71. [DOI: 10.1016/j. jjcc.2021.01.010]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
